
Page 706 - Saunders Comprehensive Review For NCLEX-RN
P. 706
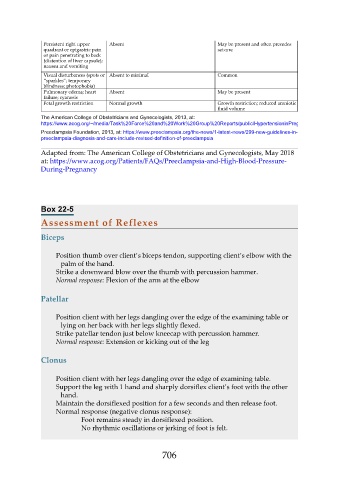
Persistent right upper Absent May be present and often precedes
quadrant or epigastric pain seizure
or pain penetrating to back
(distention of liver capsule);
nausea and vomiting
Visual disturbances (spots or Absent to minimal Common
“sparkles”; temporary
blindness; photophobia)
Pulmonary edema; heart Absent May be present
failure; cyanosis
Fetal growth restriction Normal growth Growth restriction; reduced amniotic
fluid volume
The American College of Obstetricians and Gynecologists, 2013, at:
https://www.acog.org/~/media/Task%20Force%20and%20Work%20Group%20Reports/public/HypertensioninPregnancy.pdf
Preeclampsia Foundation, 2013, at: https://www.preeclampsia.org/the-news/1-latest-news/299-new-guidelines-in-
preeclampsia-diagnosis-and-care-include-revised-definition-of-preeclampsia
Adapted from: The American College of Obstetricians and Gynecologists, May 2018
at: https://www.acog.org/Patients/FAQs/Preeclampsia-and-High-Blood-Pressure-
During-Pregnancy
Box 22-5
Assessment of Reflexes
Biceps
Position thumb over client’s biceps tendon, supporting client’s elbow with the
palm of the hand.
Strike a downward blow over the thumb with percussion hammer.
Normal response: Flexion of the arm at the elbow
Patellar
Position client with her legs dangling over the edge of the examining table or
lying on her back with her legs slightly flexed.
Strike patellar tendon just below kneecap with percussion hammer.
Normal response: Extension or kicking out of the leg
Clonus
Position client with her legs dangling over the edge of examining table.
Support the leg with 1 hand and sharply dorsiflex client’s foot with the other
hand.
Maintain the dorsiflexed position for a few seconds and then release foot.
Normal response (negative clonus response):
Foot remains steady in dorsiflexed position.
No rhythmic oscillations or jerking of foot is felt.
706