
Page 172 - Clinical Pearls in Cardiology
P. 172
160 Clinical Pearls in Cardiology
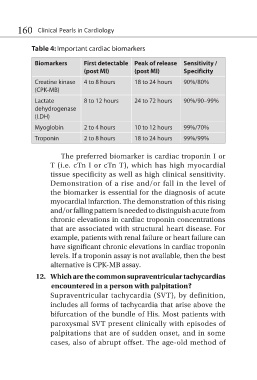
Table 4: Important cardiac biomarkers
Biomarkers First detectable Peak of release Sensitivity /
(post MI) (post MI) Specificity
Creatine kinase 4 to 8 hours 18 to 24 hours 90%/80%
(CPK-MB)
Lactate 8 to 12 hours 24 to 72 hours 90%/90–99%
dehydrogenase
(LDH)
Myoglobin 2 to 4 hours 10 to 12 hours 99%/70%
Troponin 2 to 8 hours 18 to 24 hours 99%/99%
The preferred biomarker is cardiac troponin I or
T (i.e. cTn I or cTn T), which has high myocardial
tissue specificity as well as high clinical sensitivity.
Demonstration of a rise and/or fall in the level of
the biomarker is essential for the diagnosis of acute
myocardial infarction. The demonstration of this rising
and/or falling pattern is needed to distinguish acute from
chronic elevations in cardiac troponin concentrations
that are associated with structural heart disease. For
example, patients with renal failure or heart failure can
have significant chronic elevations in cardiac troponin
levels. If a troponin assay is not available, then the best
alternative is CPK-MB assay.
12. Which are the common supraventricular tachycardias
encountered in a person with palpitation?
Supraventricular tachycardia (SVT), by definition,
includes all forms of tachycardia that arise above the
bifurcation of the bundle of His. Most patients with
paroxysmal SVT present clinically with episodes of
palpitations that are of sudden onset, and in some
cases, also of abrupt offset. The age-old method of