
Page 167 - Clinical Pearls in Cardiology
P. 167
Ischemic Heart Disease 155
4. What is the relation between the structure of
atherosclerotic plaque and its clinical outcome in a
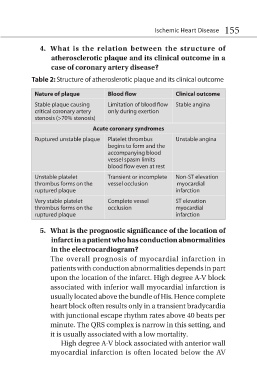
case of coronary artery disease?
Table 2: Structure of atheroslerotic plaque and its clinical outcome
Nature of plaque Blood flow Clinical outcome
Stable plaque causing Limitation of blood flow Stable angina
critical coronary artery only during exertion
stenosis (>70% stenosis)
Acute coronary syndromes
Ruptured unstable plaque Platelet thrombus Unstable angina
begins to form and the
accompanying blood
vessel spasm limits
blood flow even at rest
Unstable platelet Transient or incomplete Non-ST elevation
thrombus forms on the vessel occlusion myocardial
ruptured plaque infarction
Very stable platelet Complete vessel ST elevation
thrombus forms on the occlusion myocardial
ruptured plaque infarction
5. What is the prognostic significance of the location of
infarct in a patient who has conduction abnormalities
in the electrocardiogram?
The overall prognosis of myocardial infarction in
patients with conduction abnormalities depends in part
upon the location of the infarct. High degree A-V block
associated with inferior wall myocardial infarction is
usually located above the bundle of His. Hence complete
heart block often results only in a transient bradycardia
with junctional escape rhythm rates above 40 beats per
minute. The QRS complex is narrow in this setting, and
it is usually associated with a low mortality.
High degree A-V block associated with anterior wall
myocardial infarction is often located below the AV