
Page 94 - Clinical Pearls in Cardiology
P. 94
82 Clinical Pearls in Cardiology
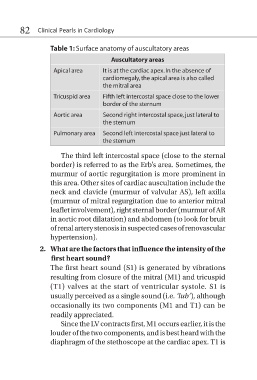
Table 1: Surface anatomy of auscultatory areas
Auscultatory areas
Apical area It is at the cardiac apex. In the absence of
cardiomegaly, the apical area is also called
the mitral area
Tricuspid area Fifth left intercostal space close to the lower
border of the sternum
Aortic area Second right intercostal space, just lateral to
the sternum
Pulmonary area Second left intercostal space just lateral to
the sternum
The third left intercostal space (close to the sternal
border) is referred to as the Erb’s area. Sometimes, the
murmur of aortic regurgitation is more prominent in
this area. Other sites of cardiac auscultation include the
neck and clavicle (murmur of valvular AS), left axilla
(murmur of mitral regurgitation due to anterior mitral
leaflet involvement), right sternal border (murmur of AR
in aortic root dilatation) and abdomen (to look for bruit
of renal artery stenosis in suspected cases of renovascular
hypertension).
2. What are the factors that influence the intensity of the
first heart sound?
The first heart sound (S1) is generated by vibrations
resulting from closure of the mitral (M1) and tricuspid
(T1) valves at the start of ventricular systole. S1 is
usually perceived as a single sound (i.e. ‘lub’), although
occasionally its two components (M1 and T1) can be
readily appreciated.
Since the LV contracts first, M1 occurs earlier, it is the
louder of the two components, and is best heard with the
diaphragm of the stethoscope at the cardiac apex. T1 is