
Page 7 - United Capital EE Guide 04-17
P. 7
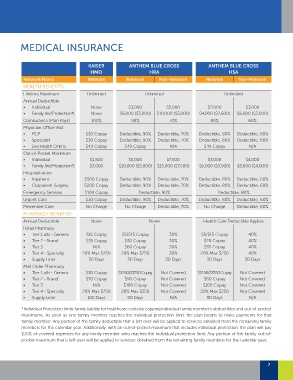
MEDICAL INSURANCE
KAISER ANTHEM BLUE CROSS ANTHEM BLUE CROSS
HMO HRA HSA
Network Name Network Network Non-Network Network Non-Network
HEALTH BENEFITS
Lifetime Maximum Unlimited Unlimited Unlimited
Annual Deductible
• Individual None $3,000 $5,000 $2,000 $3,000
• Family (Ind Protection*) None $6,000 ($3,000) $10,000 ($5,000) $4,000 ($2,600) $6,000 ($3,000)
Coinsurance (Plan Pays) 100% 90% 70% 80% 60%
Physician Office Visit
• PCP $30 Copay Deductible, 90% Deductible, 70% Deductible, 80% Deductible, 60%
• Specialist $30 Copay Deductible, 90% Deductible, 70% Deductible, 80% Deductible, 60%
• LiveHealth Online $49 Copay $49 Copay N/A $49 Copay N/A
Out-of-Pocket Maximum
• Individual $1,500 $5,000 $7,500 $3,000 $4,000
• Family (Ind Protection*) $3,000 $10,000 ($5,000) $15,000 ($7,500) $6,000 ($3,000) $8,000 ($4,000)
Hospitalization
• Inpatient $500 Copay Deductible, 90% Deductible, 70% Deductible, 80% Deductible, 60%
• Outpatient Surgery $200 Copay Deductible, 90% Deductible, 70% Deductible, 80% Deductible, 60%
Emergency Services $100 Copay Deductible, 90% Deductible, 80%
Urgent Care $30 Copay Deductible, 90% Deductible, 70% Deductible, 80% Deductible, 60%
Preventive Care No Charge No Charge Deductible, 70% No Charge Deductible, 60%
PHARMACY BENEFITS
Annual Deductible None None Health Care Deductible Applies
Retail Pharmacy
• Tier 1 a/b - Generic $15 Copay $5/$15 Copay 30% $5/$15 Copay 40%
• Tier 2 - Brand $35 Copay $30 Copay 30% $20 Copay 40%
• Tier 3 N/A $60 Copay 30% $35 Copay 40%
• Tier 4 - Specialty 20% Max $250 20% Max $250 30% 20% Max $250 40%
• Supply Limit 30 Days 30 Days 30 Days 30 Days 30 Days
Mail Order Pharmacy
• Tier 1 a/b - Generic $30 Copay $12.50/$37.50 Copay Not Covered $12.50/$37.50 Copay Not Covered
• Tier 2 - Brand $70 Copay $90 Copay Not Covered $60 Copay Not Covered
• Tier 3 N/A $180 Copay Not Covered $105 Copay Not Covered
• Tier 4 - Specialty 20% Max $250 20% Max $250 Not Covered 20% Max $250 Not Covered
• Supply Limit 100 Days 90 Days N/A 90 Days N/A
*Individual Protection limits family liability for healthcare costs by capping individual family member’s deductibles and out-of-pocket
maximums. As soon as one family member reaches the individual protection limit, the plan begins to make payments for that
family member. Any portion of the family deductible that is left over will be applied to services obtained from the remaining family
members for the calendar year. Additionally, with an out-of-pocket maximum that includes individual protection, the plan will pay
100% of covered expenses for any family member who reaches the individual protection limit. Any portion of the family out-of-
pocket maximum that is left over will be applied to services obtained from the remaining family members for the calendar year.
7