
Page 7 - Burlingame EE Guide 12-19 - English
P. 7
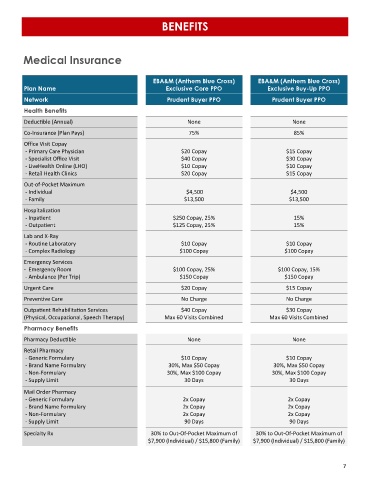
BENEFITS
Medical Insurance
EBA&M (Anthem Blue Cross) EBA&M (Anthem Blue Cross)
Plan Name Exclusive Core PPO Exclusive Buy-Up PPO
Network Prudent Buyer PPO Prudent Buyer PPO
Health Benefits
Deductible (Annual) None None
Co-Insurance (Plan Pays) 75% 85%
Office Visit Copay
- Primary Care Physician $20 Copay $15 Copay
- Specialist Office Visit $40 Copay $30 Copay
- LiveHealth Online (LHO) $10 Copay $10 Copay
- Retail Health Clinics $20 Copay $15 Copay
Out-of-Pocket Maximum
- Individual $4,500 $4,500
- Family $13,500 $13,500
Hospitalization
- Inpatient $250 Copay, 25% 15%
- Outpatient $125 Copay, 25% 15%
Lab and X-Ray
- Routine Laboratory $10 Copay $10 Copay
- Complex Radiology $100 Copay $100 Copay
Emergency Services
- Emergency Room $100 Copay, 25% $100 Copay, 15%
- Ambulance (Per Trip) $150 Copay $150 Copay
Urgent Care $20 Copay $15 Copay
Preventive Care No Charge No Charge
Outpatient Rehabilitation Services $40 Copay $30 Copay
(Physical, Occupational, Speech Therapy) Max 60 Visits Combined Max 60 Visits Combined
Pharmacy Benefits
Pharmacy Deductible None None
Retail Pharmacy
- Generic Formulary $10 Copay $10 Copay
- Brand Name Formulary 30%, Max $50 Copay 30%, Max $50 Copay
- Non-Formulary 30%, Max $100 Copay 30%, Max $100 Copay
- Supply Limit 30 Days 30 Days
Mail Order Pharmacy
- Generic Formulary 2x Copay 2x Copay
- Brand Name Formulary 2x Copay 2x Copay
- Non-Formulary 2x Copay 2x Copay
- Supply Limit 90 Days 90 Days
Specialty Rx 30% to Out-Of-Pocket Maximum of 30% to Out-Of-Pocket Maximum of
$7,900 (Individual) / $15,800 (Family) $7,900 (Individual) / $15,800 (Family)
7