
Page 7 - Westmark BG 2020
P. 7
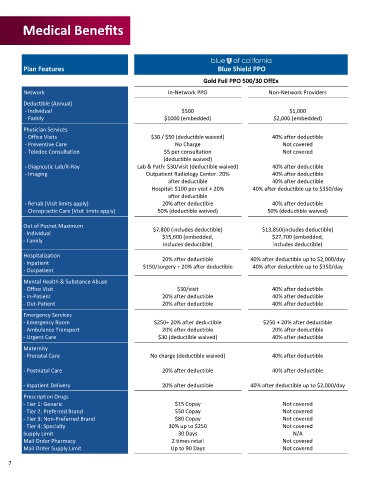
Medical Benefits
Plan Features Blue Shield PPO
Gold Full PPO 500/30 OffEx
Network In-Network PPO Non-Network Providers
Deductible (Annual)
- Individual $500 $1,000
- Family $1000 (embedded) $2,000 (embedded)
Physician Services
- Office Visits $30 / $50 (deductible waived) 40% after deductible
- Preventive Care No Charge Not covered
- Teledoc Consultation $5 per consultation Not covered
(deductible waived)
- Diagnostic Lab/X-Ray Lab & Path: $30/visit (deductible waived) 40% after deductible
- Imaging Outpatient Radiology Center: 20% 40% after deductible
after deductible 40% after deductible
Hospital: $100 per visit + 20% 40% after deductible up to $350/day
after deductible
- Rehab (Visit limits apply) 20% after deductible 40% after deductible
- Chiropractic Care (Visit limits apply) 50% (deductible waived) 50% (deductible waived)
Out of Pocket Maximum $7,800 (includes deductible) $13,850(includes deductible)
- Individual
$15,600 (embedded, $27,700 (embedded,
- Family
includes deductible) includes deductible)
Hospitalization 20% after deductible 40% after deductible up to $2,000/day
- Inpatient
$150/surgery + 20% after deductible 40% after deductible up to $350/day
- Outpatient
Mental Health & Substance Abuse
- Office Visit $30/visit 40% after deductible
- In-Patient 20% after deductible 40% after deductible
- Out-Patient 20% after deductible 40% after deductible
Emergency Services
- Emergency Room $250+ 20% after deductible $250 + 20% after deductible
- Ambulance Transport 20% after deductible 20% after deductible
- Urgent Care $30 (deductible waived) 40% after deductible
Maternity
- Prenatal Care No charge (deductible waived) 40% after deductible
- Postnatal Care 20% after deductible 40% after deductible
- Inpatient Delivery 20% after deductible 40% after deductible up to $2,000/day
Prescription Drugs
- Tier 1: Generic $15 Copay Not covered
- Tier 2: Preferred Brand $50 Copay Not covered
- Tier 3: Non-Preferred Brand $80 Copay Not covered
- Tier 4: Specialty 30% up to $250 Not covered
Supply Limit 30 Days N/A
Mail Order Pharmacy 2 times retail Not covered
Mail Order Supply Limit Up to 90 Days Not covered
7