
Page 6 - MMCS Benefit Guide 2019 FINAL
P. 6
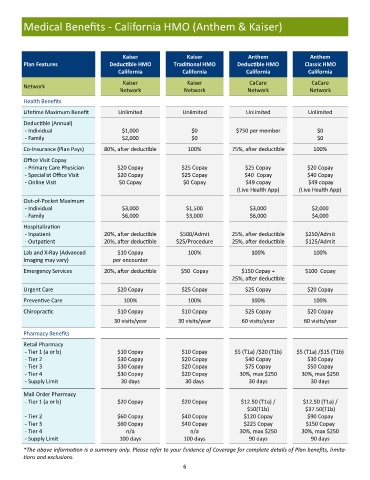
Medical Benefits - California HMO (Anthem & Kaiser)
Kaiser Kaiser Anthem Anthem
Plan Features Deductible HMO Traditional HMO Deductible HMO Classic HMO
California California California California
Kaiser Kaiser CaCare CaCare
Network
Network Network Network Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited Unlimited Unlimited
Deductible (Annual)
- Individual $1,000 $0 $750 per member $0
- Family $2,000 $0 $0
Co-Insurance (Plan Pays) 80%, after deductible 100% 75%, after deductible 100%
Office Visit Copay
- Primary Care Physician $20 Copay $25 Copay $25 Copay $20 Copay
- Specialist Office Visit $20 Copay $25 Copay $40 Copay $40 Copay
- Online Visit $0 Copay $0 Copay $49 copay $49 copay
(Live Health App) (Live Health App)
Out-of-Pocket Maximum
- Individual $3,000 $1,500 $3,000 $2,000
- Family $6,000 $3,000 $6,000 $4,000
Hospitalization
- Inpatient 20%, after deductible $500/Admit 25%, after deductible $250/Admit
- Outpatient 20%, after deductible $25/Procedure 25%, after deductible $125/Admit
Lab and X-Ray (Advanced $10 Copay 100% 100% 100%
Imaging may vary) per encounter
Emergency Services 20%, after deductible $50 Copay $150 Copay + $100 Copay
25%, after deductible
Urgent Care $20 Copay $25 Copay $25 Copay $20 Copay
Preventive Care 100% 100% 100% 100%
Chiropractic $10 Copay $10 Copay $25 Copay $20 Copay
30 visits/year 30 visits/year 60 visits/year 60 visits/year
Pharmacy Benefits
Retail Pharmacy
- Tier 1 (a or b) $10 Copay $10 Copay $5 (T1a) /$20 (T1b) $5 (T1a) /$15 (T1b)
- Tier 2 $30 Copay $20 Copay $40 Copay $30 Copay
- Tier 3 $30 Copay $20 Copay $75 Copay $50 Copay
- Tier 4 $30 Copay $20 Copay 30%, max $250 30%, max $250
- Supply Limit 30 days 30 days 30 days 30 days
Mail Order Pharmacy
- Tier 1 (a or b) $20 Copay $20 Copay $12.50 (T1a) / $12.50 (T1a) /
$50(T1b) $37.50(T1b)
- Tier 2 $60 Copay $40 Copay $120 Copay $90 Copay
- Tier 3 $60 Copay $40 Copay $225 Copay $150 Copay
- Tier 4 n/a n/a 30%, max $250 30%, max $250
- Supply Limit 100 days 100 days 90 days 90 days
*The above information is a summary only. Please refer to your Evidence of Coverage for complete details of Plan benefits, limita-
tions and exclusions.
6