
Page 7 - MMCS Benefit Guide 2019 FINAL
P. 7
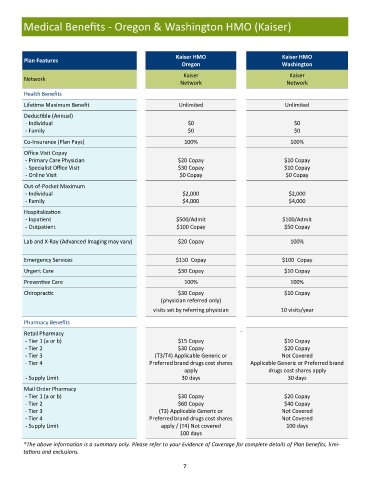
Medical Benefits - Oregon & Washington HMO (Kaiser)
Kaiser HMO Kaiser HMO
Plan Features
Oregon Washington
Kaiser Kaiser
Network
Network Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Deductible (Annual)
- Individual $0 $0
- Family $0 $0
Co-Insurance (Plan Pays) 100% 100%
Office Visit Copay
- Primary Care Physician $20 Copay $10 Copay
- Specialist Office Visit $30 Copay $10 Copay
- Online Visit $0 Copay $0 Copay
Out-of-Pocket Maximum
- Individual $2,000 $2,000
- Family $4,000 $4,000
Hospitalization
- Inpatient $500/Admit $100/Admit
- Outpatient $100 Copay $50 Copay
Lab and X-Ray (Advanced Imaging may vary) $20 Copay 100%
Emergency Services $150 Copay $100 Copay
Urgent Care $30 Copay $10 Copay
Preventive Care 100% 100%
Chiropractic $30 Copay $10 Copay
(physician referred only)
visits set by referring physician 10 visits/year
Pharmacy Benefits
Retail Pharmacy `
- Tier 1 (a or b) $15 Copay $10 Copay
- Tier 2 $30 Copay $20 Copay
- Tier 3 (T3/T4) Applicable Generic or Not Covered
- Tier 4 Preferred brand drugs cost shares Applicable Generic or Preferred brand
apply drugs cost shares apply
- Supply Limit 30 days 30 days
Mail Order Pharmacy
- Tier 1 (a or b) $30 Copay $20 Copay
- Tier 2 $60 Copay $40 Copay
- Tier 3 (T3) Applicable Generic or Not Covered
- Tier 4 Preferred brand drugs cost shares Not Covered
- Supply Limit apply / (T4) Not covered 100 days
100 days
*The above information is a summary only. Please refer to your Evidence of Coverage for complete details of Plan benefits, limi-
tations and exclusions.
7