
Page 8 - Palomar EE Guide 01-19 FINAL
P. 8
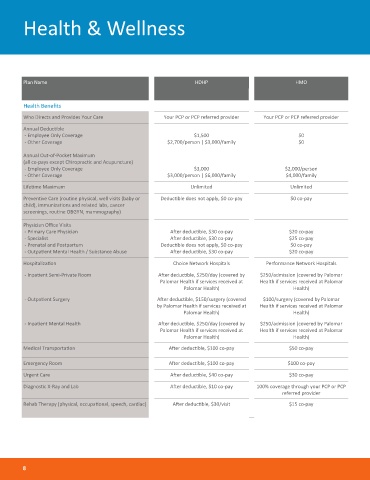
Health & Wellness
Plan Name HDHP HMO
Health Benefits
Who Directs and Provides Your Care Your PCP or PCP referred provider Your PCP or PCP referred provider
Annual Deductible
- Employee Only Coverage $1,500 $0
- Other Coverage $2,700/person | $3,000/family $0
Annual Out-of-Pocket Maximum
(all co-pays except Chiropractic and Acupuncture)
- Employee Only Coverage $3,000 $2,000/person
- Other Coverage $3,000/person | $6,000/family $4,000/family
Lifetime Maximum Unlimited Unlimited
Preventive Care (routine physical, well visits (baby or Deductible does not apply, $0 co-pay $0 co-pay
child), immunizations and related labs, cancer
screenings, routine OBGYN, mammography)
Physician Office Visits
- Primary Care Physician After deductible, $30 co-pay $20 co-pay
- Specialist After deductible, $30 co-pay $25 co-pay
- Prenatal and Postpartum Deductible does not apply, $0 co-pay $0 co-pay
- Outpatient Mental Health / Substance Abuse After deductible, $30 co-pay $20 co-pay
Hospitalization Choice Network Hospitals Performance Network Hospitals
- Inpatient Semi-Private Room After deductible, $250/day (covered by $250/admission (covered by Palomar
Palomar Health if services received at Health if services received at Palomar
Palomar Health) Health)
- Outpatient Surgery After deductible, $150/surgery (covered $100/surgery (covered by Palomar
by Palomar Health if services received at Health if services received at Palomar
Palomar Health) Health)
- Inpatient Mental Health After deductible, $250/day (covered by $250/admission (covered by Palomar
Palomar Health if services received at Health if services received at Palomar
Palomar Health) Health)
Medical Transportation After deductible, $100 co-pay $50 co-pay
Emergency Room After deductible, $100 co-pay $100 co-pay
Urgent Care After deductible, $40 co-pay $30 co-pay
Diagnostic X-Ray and Lab After deductible, $10 co-pay 100% coverage through your PCP or PCP
referred provider
Rehab Therapy (physical, occupational, speech, cardiac) After deductible, $30/visit $15 co-pay
8