
Page 7 - Redbarn Pet Products BG 2018 V5
P. 7
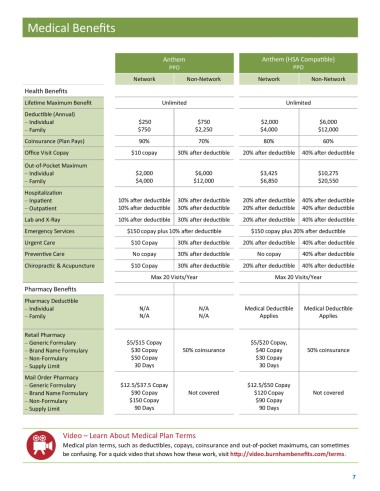
Medical Benefits
Anthem Anthem (HSA Compatible)
PPO PPO
Network Non-Network Network Non-Network
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Deductible (Annual)
Individual $250 $750 $2,000 $6,000
Family $750 $2,250 $4,000 $12,000
Coinsurance (Plan Pays) 90% 70% 80% 60%
Office Visit Copay $10 copay 30% after deductible 20% after deductible 40% after deductible
Out-of-Pocket Maximum
Individual $2,000 $6,000 $3,425 $10,275
Family $4,000 $12,000 $6,850 $20,550
Hospitalization
Inpatient 10% after deductible 30% after deductible 20% after deductible 40% after deductible
Outpatient 10% after deductible 30% after deductible 20% after deductible 40% after deductible
Lab and X-Ray 10% after deductible 30% after deductible 20% after deductible 40% after deductible
Emergency Services $150 copay plus 10% after deductible $150 copay plus 20% after deductible
Urgent Care $10 Copay 30% after deductible 20% after deductible 40% after deductible
Preventive Care No copay 30% after deductible No copay 40% after deductible
Chiropractic & Acupuncture $10 Copay 30% after deductible 20% after deductible 40% after deductible
Max 20 Visits/Year Max 20 Visits/Year
Pharmacy Benefits
Pharmacy Deductible
Individual N/A N/A Medical Deductible Medical Deductible
Family N/A N/A Applies Applies
Retail Pharmacy
Generic Formulary $5/$15 Copay $5/$20 Copay,
Brand Name Formulary $30 Copay 50% coinsurance $40 Copay 50% coinsurance
Non-Formulary $50 Copay $30 Copay
Supply Limit 30 Days 30 Days
Mail Order Pharmacy
Generic Formulary $12.5/$37.5 Copay $12.5/$50 Copay
Brand Name Formulary $90 Copay Not covered $120 Copay Not covered
Non-Formulary $150 Copay $90 Copay
Supply Limit 90 Days 90 Days
Video – Learn About Medical Plan Terms
Medical plan terms, such as deductibles, copays, coinsurance and out-of-pocket maximums, can sometimes
be confusing. For a quick video that shows how these work, visit http://video.burnhambenefits.com/terms.
7