
Page 9 - Alexander EE Guide 01- 20
P. 9
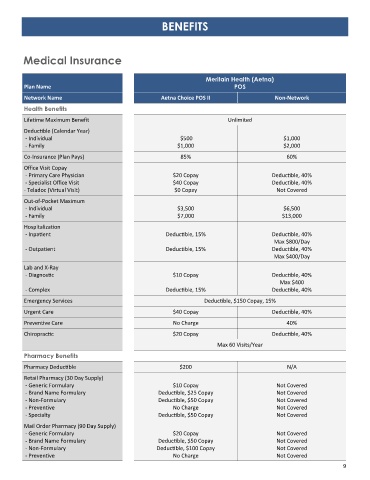
BENEFITS
Medical Insurance
Meritain Health (Aetna)
Plan Name POS
Network Name Aetna Choice POS II Non-Network
Health Benefits
Lifetime Maximum Benefit Unlimited
Deductible (Calendar Year)
- Individual $500 $1,000
- Family $1,000 $2,000
Co-Insurance (Plan Pays) 85% 60%
Office Visit Copay
- Primary Care Physician $20 Copay Deductible, 40%
- Specialist Office Visit $40 Copay Deductible, 40%
- Teladoc (Virtual Visit) $0 Copay Not Covered
Out-of-Pocket Maximum
- Individual $3,500 $6,500
- Family $7,000 $13,000
Hospitalization
- Inpatient Deductible, 15% Deductible, 40%
Max $800/Day
- Outpatient Deductible, 15% Deductible, 40%
Max $400/Day
Lab and X-Ray
- Diagnostic $10 Copay Deductible, 40%
Max $400
- Complex Deductible, 15% Deductible, 40%
Emergency Services Deductible, $150 Copay, 15%
Urgent Care $40 Copay Deductible, 40%
Preventive Care No Charge 40%
Chiropractic $20 Copay Deductible, 40%
Max 60 Visits/Year
Pharmacy Benefits
Pharmacy Deductible $200 N/A
Retail Pharmacy (30 Day Supply)
- Generic Formulary $10 Copay Not Covered
- Brand Name Formulary Deductible, $25 Copay Not Covered
- Non-Formulary Deductible, $50 Copay Not Covered
- Preventive No Charge Not Covered
- Specialty Deductible, $50 Copay Not Covered
Mail Order Pharmacy (90 Day Supply)
- Generic Formulary $20 Copay Not Covered
- Brand Name Formulary Deductible, $50 Copay Not Covered
- Non-Formulary Deductible, $100 Copay Not Covered
- Preventive No Charge Not Covered
9