
Page 8 - Alexander EE Guide 01- 20
P. 8
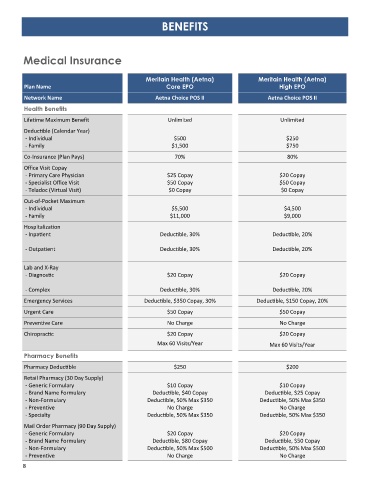
BENEFITS
Medical Insurance
Meritain Health (Aetna) Meritain Health (Aetna)
Plan Name Core EPO High EPO
Network Name Aetna Choice POS II Aetna Choice POS II
Health Benefits
Lifetime Maximum Benefit Unlimited Unlimited
Deductible (Calendar Year)
- Individual $500 $250
- Family $1,500 $750
Co-Insurance (Plan Pays) 70% 80%
Office Visit Copay
- Primary Care Physician $25 Copay $20 Copay
- Specialist Office Visit $50 Copay $50 Copay
- Teladoc (Virtual Visit) $0 Copay $0 Copay
Out-of-Pocket Maximum
- Individual $5,500 $4,500
- Family $11,000 $9,000
Hospitalization
- Inpatient Deductible, 30% Deductible, 20%
- Outpatient Deductible, 30% Deductible, 20%
Lab and X-Ray
- Diagnostic $20 Copay $20 Copay
- Complex Deductible, 30% Deductible, 20%
Emergency Services Deductible, $350 Copay, 30% Deductible, $150 Copay, 20%
Urgent Care $50 Copay $50 Copay
Preventive Care No Charge No Charge
Chiropractic $20 Copay $20 Copay
Max 60 Visits/Year Max 60 Visits/Year
Pharmacy Benefits
Pharmacy Deductible $250 $200
Retail Pharmacy (30 Day Supply)
- Generic Formulary $10 Copay $10 Copay
- Brand Name Formulary Deductible, $40 Copay Deductible, $25 Copay
- Non-Formulary Deductible, 50% Max $350 Deductible, 50% Max $350
- Preventive No Charge No Charge
- Specialty Deductible, 50% Max $350 Deductible, 50% Max $350
Mail Order Pharmacy (90 Day Supply)
- Generic Formulary $20 Copay $20 Copay
- Brand Name Formulary Deductible, $80 Copay Deductible, $50 Copay
- Non-Formulary Deductible, 50% Max $500 Deductible, 50% Max $500
- Preventive No Charge No Charge
8