
Page 10 - Parsons and Parsons Corp ODD EE Guide 1 1 17_FINAL 11.1.16
P. 10
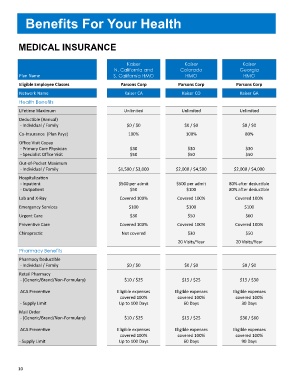
Benefits For Your Health
MEDICAL INSURANCE
Kaiser Kaiser Kaiser
N. California and Colorado Georgia
Plan Name S. California HMO HMO HMO
Eligible Employee Classes Parsons Corp Parsons Corp Parsons Corp
Network Name Kaiser CA Kaiser CO Kaiser GA
Health Benefits
Lifetime Maximum Unlimited Unlimited Unlimited
Deductible (Annual)
- Individual / Family $0 / $0 $0 / $0 $0 / $0
Co-Insurance (Plan Pays) 100% 100% 80%
Office Visit Copay
- Primary Care Physician $30 $30 $30
- Specialist Office Visit $50 $50 $50
Out-of-Pocket Maximum
- Individual / Family $1,500 / $3,000 $2,000 / $4,500 $2,000 / $4,000
Hospitalization
- Inpatient $500 per admit $500 per admit 80% after deductible
- Outpatient $50 $100 80% after deductible
Lab and X-Ray Covered 100% Covered 100% Covered 100%
Emergency Services $100 $100 $100
Urgent Care $30 $50 $60
Preventive Care Covered 100% Covered 100% Covered 100%
Chiropractic Not covered $30 $50
20 Visits/Year 20 Visits/Year
Pharmacy Benefits
Pharmacy Deductible
- Individual / Family $0 / $0 $0 / $0 $0 / $0
Retail Pharmacy
- (Generic/Brand/Non-Formulary) $10 / $25 $15 / $25 $15 / $30
ACA Preventive Eligible expenses Eligible expenses Eligible expenses
covered 100% covered 100% covered 100%
- Supply Limit Up to 100 Days 60 Days 30 Days
Mail Order
- (Generic/Brand/Non-Formulary) $10 / $25 $15 / $25 $30 / $60
ACA Preventive Eligible expenses Eligible expenses Eligible expenses
covered 100% covered 100% covered 100%
- Supply Limit Up to 100 Days 60 Days 90 Days
10