
Page 7 - SBCEO Benefit Guide 19-20_FINAL
P. 7
Employee Contributions 7
Health Benefit Contributions For Full-Time Employees
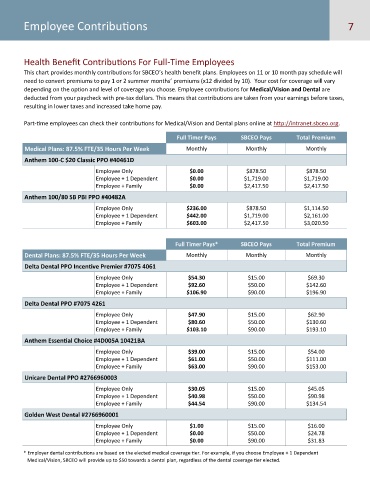
This chart provides monthly contributions for SBCEO’s health benefit plans. Employees on 11 or 10 month pay schedule will
need to convert premiums to pay 1 or 2 summer months’ premiums (x12 divided by 10). Your cost for coverage will vary
depending on the option and level of coverage you choose. Employee contributions for Medical/Vision and Dental are
deducted from your paycheck with pre-tax dollars. This means that contributions are taken from your earnings before taxes,
resulting in lower taxes and increased take home pay.
Part-time employees can check their contributions for Medical/Vision and Dental plans online at http://intranet.sbceo.org.
Full Timer Pays SBCEO Pays Total Premium
Medical Plans: 87.5% FTE/35 Hours Per Week Monthly Monthly Monthly
Anthem 100-C $20 Classic PPO #40461D
Employee Only $0.00 $878.50 $878.50
Employee + 1 Dependent $0.00 $1,719.00 $1,719.00
Employee + Family $0.00 $2,417.50 $2,417.50
Anthem 100/80 SB PBI PPO #40482A
Employee Only $236.00 $878.50 $1,114.50
Employee + 1 Dependent $442.00 $1,719.00 $2,161.00
Employee + Family $603.00 $2,417.50 $3,020.50
Full Timer Pays* SBCEO Pays Total Premium
Dental Plans: 87.5% FTE/35 Hours Per Week Monthly Monthly Monthly
Delta Dental PPO Incentive Premier #7075 4061
Employee Only $54.30 $15.00 $69.30
Employee + 1 Dependent $92.60 $50.00 $142.60
Employee + Family $106.90 $90.00 $196.90
Delta Dental PPO #7075 4261
Employee Only $47.90 $15.00 $62.90
Employee + 1 Dependent $80.60 $50.00 $130.60
Employee + Family $103.10 $90.00 $193.10
Anthem Essential Choice #4D005A 10421BA
Employee Only $39.00 $15.00 $54.00
Employee + 1 Dependent $61.00 $50.00 $111.00
Employee + Family $63.00 $90.00 $153.00
Unicare Dental PPO #2766960003
Employee Only $30.05 $15.00 $45.05
Employee + 1 Dependent $40.98 $50.00 $90.98
Employee + Family $44.54 $90.00 $134.54
Golden West Dental #2766960001
Employee Only $1.00 $15.00 $16.00
Employee + 1 Dependent $0.00 $50.00 $24.78
Employee + Family $0.00 $90.00 $31.83
* Employer dental contributions are based on the elected medical coverage tier. For example, if you choose Employee + 1 Dependent
Medical/Vision, SBCEO will provide up to $50 towards a dental plan, regardless of the dental coverage tier elected.