
Page 6 - OrangeTheory Benefits Guide 07-2019_FINAL - NonCA
P. 6
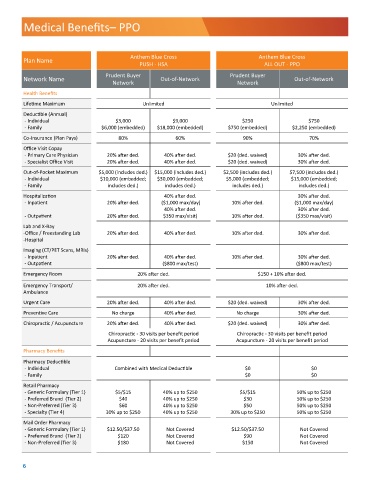
Medical Benefits– PPO
Anthem Blue Cross Anthem Blue Cross
Plan Name
PUSH - HSA ALL OUT - PPO
Prudent Buyer Prudent Buyer
Network Name Out-of-Network Out-of-Network
Network Network
Health Benefits
Lifetime Maximum Unlimited Unlimited
Deductible (Annual)
- Individual $3,000 $9,000 $250 $750
- Family $6,000 (embedded) $18,000 (embedded) $750 (embedded) $2,250 (embedded)
Co-Insurance (Plan Pays) 80% 60% 90% 70%
Office Visit Copay
- Primary Care Physician 20% after ded. 40% after ded. $20 (ded. waived) 30% after ded.
- Specialist Office Visit 20% after ded. 40% after ded. $20 (ded. waived) 30% after ded.
Out-of-Pocket Maximum $5,000 (includes ded.) $15,000 (includes ded.) $2,500 (includes ded.) $7,500 (includes ded.)
- Individual $10,000 (embedded; $30,000 (embedded; $5,000 (embedded; $15,000 (embedded;
- Family includes ded.) includes ded.) includes ded.) includes ded.)
Hospitalization 40% after ded. 30% after ded.
- Inpatient 20% after ded. ($1,000 max/day) 10% after ded. ($1,000 max/day)
40% after ded. 30% after ded.
- Outpatient 20% after ded. $350 max/visit) 10% after ded. ($350 max/visit)
Lab and X-Ray
-Office / Freestanding Lab 20% after ded. 40% after ded. 10% after ded. 30% after ded.
-Hospital
Imaging (CT/PET Scans, MRIs)
- Inpatient 20% after ded. 40% after ded. 10% after ded. 30% after ded.
- Outpatient ($800 max/test) ($800 max/test)
Emergency Room 20% after ded. $150 + 10% after ded.
Emergency Transport/ 20% after ded. 10% after ded.
Ambulance
Urgent Care 20% after ded. 40% after ded. $20 (ded. waived) 30% after ded.
Preventive Care No charge 40% after ded. No charge 30% after ded.
Chiropractic / Acupuncture 20% after ded. 40% after ded. $20 (ded. waived) 30% after ded.
Chiropractic - 30 visits per benefit period Chiropractic - 30 visits per benefit period
Acupuncture - 20 visits per benefit period Acupuncture - 20 visits per benefit period
Pharmacy Benefits
Pharmacy Deductible
- Individual Combined with Medical Deductible $0 $0
- Family $0 $0
Retail Pharmacy
- Generic Formulary (Tier 1) $5/$15 40% up to $250 $5/$15 50% up to $250
- Preferred Brand (Tier 2) $40 40% up to $250 $30 50% up to $250
- Non-Preferred (Tier 3) $60 40% up to $250 $50 50% up to $250
- Specialty (Tier 4) 30% up to $250 40% up to $250 30% up to $250 50% up to $250
Mail Order Pharmacy
- Generic Formulary (Tier 1) $12.50/$37.50 Not Covered $12.50/$37.50 Not Covered
- Preferred Brand (Tier 2) $120 Not Covered $90 Not Covered
- Non-Preferred (Tier 3) $180 Not Covered $150 Not Covered
6