
Page 17 - Work Life and Benefits Booklet 2020 SS
P. 17
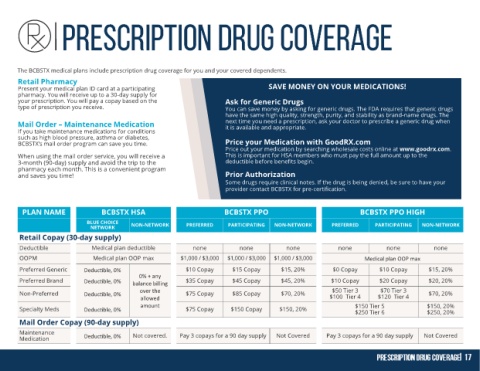
The BCBSTX medical plans include prescription drug coverage for you and your covered dependents.
Retail Pharmacy
Present your medical plan ID card at a participating SAVE MONEY ON YOUR MEDICATIONS!
pharmacy. You will receive up to a 30-day supply for
your prescription. You will pay a copay based on the Ask for Generic Drugs
type of prescription you receive. You can save money by asking for generic drugs. The FDA requires that generic drugs
have the same high quality, strength, purity, and stability as brand-name drugs. The
Mail Order – Maintenance Medication next time you need a prescription, ask your doctor to prescribe a generic drug when
it is available and appropriate.
If you take maintenance medications for conditions
such as high blood pressure, asthma or diabetes,
BCBSTX’s mail order program can save you time. Price your Medication with GoodRX.com
Price out your medication by searching wholesale costs online at www.goodrx.com.
When using the mail order service, you will receive a This is important for HSA members who must pay the full amount up to the
3-month (90-day) supply and avoid the trip to the deductible before benefits begin.
pharmacy each month. This is a convenient program
and saves you time! Prior Authorization
Some drugs require clinical notes. If the drug is being denied, be sure to have your
provider contact BCBSTX for pre-certification.
PLAN NAME BCBSTX HSA BCBSTX PPO BCBSTX PPO HIGH
BLUE CHOICE NON-NETWORK PREFERRED PARTICIPATING NON-NETWORK PREFERRED PARTICIPATING NON-NETWORK
NETWORK
Retail Copay (30-day supply)
Deductible Medical plan deductible none none none none none none
OOPM Medical plan OOP max $1,000 / $3,000 $1,000 / $3,000 $1,000 / $3,000 Medical plan OOP max
Preferred Generic Deductible, 0% $10 Copay $15 Copay $15, 20% $0 Copay $10 Copay $15, 20%
0% + any
Preferred Brand Deductible, 0% $35 Copay $45 Copay $45, 20% $10 Copay $20 Copay $20, 20%
balance billing
Non-Preferred Deductible, 0% over the $75 Copay $85 Copay $70, 20% $50 Tier 3 $70 Tier 3 $70, 20%
allowed $100 Tier 4 $120 Tier 4
Specialty Meds Deductible, 0% amount $75 Copay $150 Copay $150, 20% $150 Tier 5 $150, 20%
$250 Tier 6
$250, 20%
Mail Order Copay (90-day supply)
Maintenance Not covered. Pay 3 copays for a 90 day supply Not Covered Pay 3 copays for a 90 day supply Not Covered
Medication Deductible, 0%