
Page 202 - Essential Haematology
P. 202
188 / Chapter 13 Acute myeloid leukaemia
Chemotherapy Induction Consolidation 1 Consolidation 2 Consolidation 3
e.g. m-amasacrine,
as induction
daunorubicin,
e.g. mitoxantrone,
cytosine
high dose cytosine
cytosine
arabinoside,
arabinoside,
arabinoside,
etoposide
etoposide
idarubicin
Platelet
Support transfusions
care
Packed red cell
transfusions
16
Haemoglobin (g/dL) 12 8
4
Bone
marrow 90% <5% <5% <5% <5%
blasts
300 Platelets
White cell/platelet counts (x 10 9 /L) 10 5 1 neutrophils Total WBC
100
50
Total
0.5
0.1
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Time (weeks)
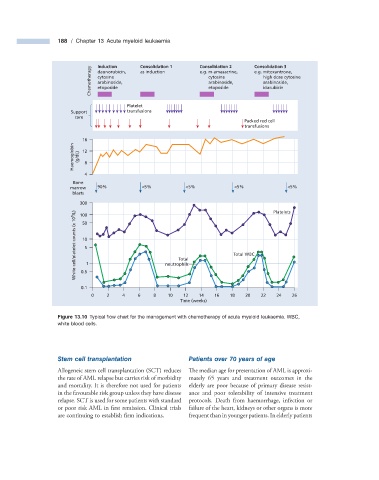
Figure 13.10 Typical fl ow chart for the management with chemotherapy of acute myeloid leukaemia. WBC,
white blood cells.
Stem c ell t ransplantation Patients over 70 y ears of a ge
Allogeneic stem cell transplantation (SCT) reduces The median age for presentation of AML is approxi-
the rate of AML relapse but carries risk of morbidity mately 65 years and treatment outcomes in the
and mortality. It is therefore not used for patients elderly are poor because of primary disease resist-
in the favourable risk group unless they have disease ance and poor tolerability of intensive treatment
relapse. SCT is used for some patients with standard protocols. Death from haemorrhage, infection or
or poor risk AML in first remission. Clinical trials failure of the heart, kidneys or other organs is more
are continuing to establish fi rm indications. frequent than in younger patients. In elderly patients