
Page 694 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 694
680 SECTION VII Endocrine Drugs
A Dopamine agonist therapy during the early weeks of pregnancy
120 has not been associated with an increased risk of spontaneous
Serum prolactin (mcg/liter) 80 pregnancy, there is growing evidence that cabergoline is also safe
abortion or congenital malformations. Although there has been
100
a longer experience with the safety of bromocriptine during early
in women with macroadenomas who must continue a dopamine
60
agonist during pregnancy. In patients with small pituitary adeno-
40
mas, dopamine agonist therapy is discontinued upon conception
20
Patients with very large adenomas require vigilance for tumor
0
0 2 4 6 8 10 12 14 16 18 20 22 24 because growth of microadenomas during pregnancy is rare.
progression and often require a dopamine agonist throughout
Weeks of cabergoline therapy pregnancy. There have been rare reports of stroke or coronary
B
thrombosis in postpartum women taking bromocriptine to
100 suppress postpartum lactation.
80
% of patients 60 ■ POSTERIOR PITUITARY
HORMONES
40
20
The two posterior pituitary hormones—vasopressin and oxytocin—
0 are synthesized in neuronal cell bodies in the hypothalamus and
Complete Partial Failure transported via their axons to the posterior pituitary, where they are
success success
stored and then released into the circulation. Each has limited but
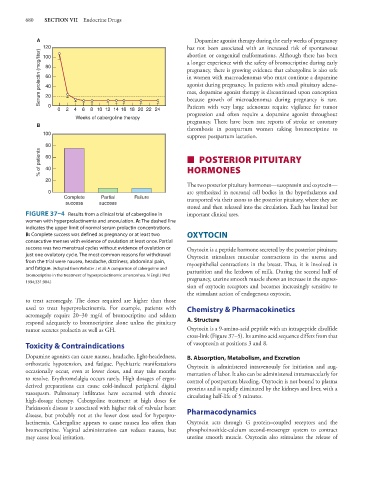
FIGURE 37–4 Results from a clinical trial of cabergoline in important clinical uses.
women with hyperprolactinemia and anovulation. A: The dashed line
indicates the upper limit of normal serum prolactin concentrations.
B: Complete success was defined as pregnancy or at least two OXYTOCIN
consecutive menses with evidence of ovulation at least once. Partial
success was two menstrual cycles without evidence of ovulation or Oxytocin is a peptide hormone secreted by the posterior pituitary.
just one ovulatory cycle. The most common reasons for withdrawal Oxytocin stimulates muscular contractions in the uterus and
from the trial were nausea, headache, dizziness, abdominal pain, myoepithelial contractions in the breast. Thus, it is involved in
and fatigue. (Adapted from Webster J et al: A comparison of cabergoline and parturition and the letdown of milk. During the second half of
bromocriptine in the treatment of hyperprolactinemic amenorrhea. N Engl J Med pregnancy, uterine smooth muscle shows an increase in the expres-
1994;331:904.)
sion of oxytocin receptors and becomes increasingly sensitive to
the stimulant action of endogenous oxytocin.
to treat acromegaly. The doses required are higher than those
used to treat hyperprolactinemia. For example, patients with Chemistry & Pharmacokinetics
acromegaly require 20–30 mg/d of bromocriptine and seldom
respond adequately to bromocriptine alone unless the pituitary A. Structure
tumor secretes prolactin as well as GH. Oxytocin is a 9-amino-acid peptide with an intrapeptide disulfide
cross-link (Figure 37–5). Its amino acid sequence differs from that
Toxicity & Contraindications of vasopressin at positions 3 and 8.
Dopamine agonists can cause nausea, headache, light-headedness, B. Absorption, Metabolism, and Excretion
orthostatic hypotension, and fatigue. Psychiatric manifestations Oxytocin is administered intravenously for initiation and aug-
occasionally occur, even at lower doses, and may take months mentation of labor. It also can be administered intramuscularly for
to resolve. Erythromelalgia occurs rarely. High dosages of ergot- control of postpartum bleeding. Oxytocin is not bound to plasma
derived preparations can cause cold-induced peripheral digital proteins and is rapidly eliminated by the kidneys and liver, with a
vasospasm. Pulmonary infiltrates have occurred with chronic circulating half-life of 5 minutes.
high-dosage therapy. Cabergoline treatment at high doses for
Parkinson’s disease is associated with higher risk of valvular heart Pharmacodynamics
disease, but probably not at the lower dose used for hyperpro-
lactinemia. Cabergoline appears to cause nausea less often than Oxytocin acts through G protein–coupled receptors and the
bromocriptine. Vaginal administration can reduce nausea, but phosphoinositide-calcium second-messenger system to contract
may cause local irritation. uterine smooth muscle. Oxytocin also stimulates the release of