
Page 703 - Basic _ Clinical Pharmacology ( PDFDrive )
P. 703
CHAPTER 38 Thyroid & Antithyroid Drugs 689
I I INACTIVATION
NH 2
Deamination
HO O CH 2 CH Decarboxylation
Conjugation
COOH (glucuronide or
I I sulfate)
Thyroxine
Deiodination
Activation Inactivation
I I
NH 2 NH 2
HO O CH 2 CH HO O CH 2 CH
COOH COOH
I I I I
3,5,3′-Triiodothyronine 3,3′,5′-Triiodothyronine
(T 3 ) (reverse T 3 )
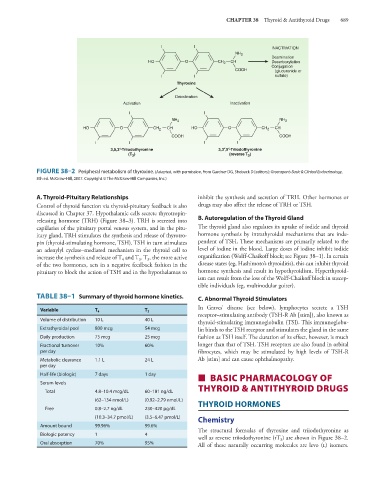
FIGURE 38–2 Peripheral metabolism of thyroxine. (Adapted, with permission, from Gardner DG, Shoback D [editors]: Greenspan’s Basic & Clinical Endocrinology,
8th ed. McGraw-Hill, 2007. Copyright © The McGraw-Hill Companies, Inc.)
A. Thyroid-Pituitary Relationships inhibit the synthesis and secretion of TRH. Other hormones or
Control of thyroid function via thyroid-pituitary feedback is also drugs may also affect the release of TRH or TSH.
discussed in Chapter 37. Hypothalamic cells secrete thyrotropin-
releasing hormone (TRH) (Figure 38–3). TRH is secreted into B. Autoregulation of the Thyroid Gland
capillaries of the pituitary portal venous system, and in the pitu- The thyroid gland also regulates its uptake of iodide and thyroid
itary gland, TRH stimulates the synthesis and release of thyrotro- hormone synthesis by intrathyroidal mechanisms that are inde-
pin (thyroid-stimulating hormone, TSH). TSH in turn stimulates pendent of TSH. These mechanisms are primarily related to the
an adenylyl cyclase–mediated mechanism in the thyroid cell to level of iodine in the blood. Large doses of iodine inhibit iodide
increase the synthesis and release of T and T . T , the more active organification (Wolff-Chaikoff block; see Figure 38–1). In certain
4
3
3
of the two hormones, acts in a negative feedback fashion in the disease states (eg, Hashimoto’s thyroiditis), this can inhibit thyroid
pituitary to block the action of TSH and in the hypothalamus to hormone synthesis and result in hypothyroidism. Hyperthyroid-
ism can result from the loss of the Wolff-Chaikoff block in suscep-
tible individuals (eg, multinodular goiter).
TABLE 38–1 Summary of thyroid hormone kinetics. C. Abnormal Thyroid Stimulators
Variable T 4 T 3 In Graves’ disease (see below), lymphocytes secrete a TSH
receptor–stimulating antibody (TSH-R Ab [stim]), also known as
Volume of distribution 10 L 40 L
thyroid-stimulating immunoglobulin (TSI). This immunoglobu-
Extrathyroidal pool 800 mcg 54 mcg lin binds to the TSH receptor and stimulates the gland in the same
Daily production 75 mcg 25 mcg fashion as TSH itself. The duration of its effect, however, is much
Fractional turnover 10% 60% longer than that of TSH. TSH receptors are also found in orbital
per day fibrocytes, which may be stimulated by high levels of TSH-R
Metabolic clearance 1.1 L 24 L Ab [stim] and can cause ophthalmopathy.
per day
Half-life (biologic) 7 days 1 day ■ BASIC PHARMACOLOGY OF
Serum levels
Total 4.8–10.4 mcg/dL 60–181 ng/dL THYROID & ANTITHYROID DRUGS
(62–134 nmol/L) (0.92–2.79 nmol/L) THYROID HORMONES
Free 0.8–2.7 ng/dL 230–420 pg/dL
(10.3–34.7 pmol/L) (3.5–6.47 pmol/L) Chemistry
Amount bound 99.96% 99.6%
The structural formulas of thyroxine and triiodothyronine as
Biologic potency 1 4
well as reverse triiodothyronine (rT ) are shown in Figure 38–2.
3
Oral absorption 70% 95% All of these naturally occurring molecules are levo (l) isomers.