Page 20 - Franklin Madison 2022 Benefits Guide
P. 20
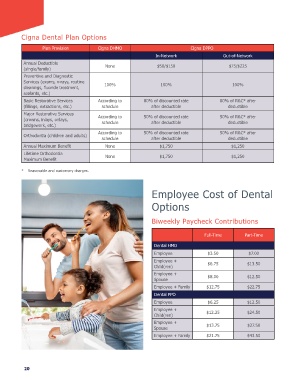
Cigna Dental Plan Options
Plan Provision Cigna DHMO Cigna DPPO
In-Network Out-of-Network
Annual Deductible None $50/$150 $75/$225
(single/family)
Preventive and Diagnostic
Services (exams, x-rays, routine 100% 100% 100%
cleanings, luoride treatment,
sealants, etc.)
Basic Restorative Services According to 80% of discounted rate 80% of R&C* after
(illings, extractions, etc.) schedule after deductible deductible
Major Restorative Services According to 50% of discounted rate 50% of R&C* after
(crowns, inlays, onlays, schedule after deductible deductible
bridgework, etc.)
Orthodontia (children and adults) According to 50% of discounted rate 50% of R&C* after
deductible
schedule
after deductible
Annual Maximum Beneit None $1,750 $1,250
Lifetime Orthodontia None $1,750 $1,250
Maximum Beneit
* Reasonable and customary charges.
Employee Cost of Dental
Options
Biweekly Paycheck Contributions
Full-Time Part-Time
Dental HMO
Employee $3.50 $7.00
Employee + $6.75 $13.50
Child(ren)
Employee + $8.00 $12.50
Spouse
Employee + Family $12.75 $22.75
Dental PPO
Employee $6.25 $12.50
Employee + $12.25 $24.50
Child(ren)
Employee + $13.75 $27.50
Spouse
Employee + Family $21.75 $43.50
20
Plan Provision Cigna DHMO Cigna DPPO
In-Network Out-of-Network
Annual Deductible None $50/$150 $75/$225
(single/family)
Preventive and Diagnostic
Services (exams, x-rays, routine 100% 100% 100%
cleanings, luoride treatment,
sealants, etc.)
Basic Restorative Services According to 80% of discounted rate 80% of R&C* after
(illings, extractions, etc.) schedule after deductible deductible
Major Restorative Services According to 50% of discounted rate 50% of R&C* after
(crowns, inlays, onlays, schedule after deductible deductible
bridgework, etc.)
Orthodontia (children and adults) According to 50% of discounted rate 50% of R&C* after
deductible
schedule
after deductible
Annual Maximum Beneit None $1,750 $1,250
Lifetime Orthodontia None $1,750 $1,250
Maximum Beneit
* Reasonable and customary charges.
Employee Cost of Dental
Options
Biweekly Paycheck Contributions
Full-Time Part-Time
Dental HMO
Employee $3.50 $7.00
Employee + $6.75 $13.50
Child(ren)
Employee + $8.00 $12.50
Spouse
Employee + Family $12.75 $22.75
Dental PPO
Employee $6.25 $12.50
Employee + $12.25 $24.50
Child(ren)
Employee + $13.75 $27.50
Spouse
Employee + Family $21.75 $43.50
20