
Page 15 - 2022 Iodine Software Benefit Guide
P. 15
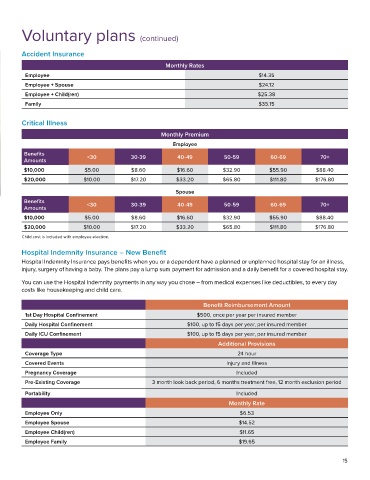
Voluntary plans (continued)
Accident Insurance
Monthly Rates
Employee $14.35
Employee + Spouse $24.12
Employee + Child(ren) $25.38
Family $35.15
Critical Illness
Monthly Premium
Employee
Benefits <30 30-39 40-49 50-59 60-69 70+
Amounts
$10,000 $5.00 $8.60 $16.60 $32.90 $55.90 $88.40
$20,000 $10.00 $17.20 $33.20 $65.80 $111.80 $176.80
Spouse
Benefits
Amounts <30 30-39 40-49 50-59 60-69 70+
$10,000 $5.00 $8.60 $16.60 $32.90 $55.90 $88.40
$20,000 $10.00 $17.20 $33.20 $65.80 $111.80 $176.80
Child cost is included with employee election.
Hospital Indemnity Insurance – New Benefit
Hospital Indemnity Insurance pays benefits when you or a dependent have a planned or unplanned hospital stay for an illness,
injury, surgery of having a baby. The plans pay a lump sum payment for admission and a daily benefit for a covered hospital stay.
You can use the Hospital Indemnity payments in any way you chose – from medical expenses like deductibles, to every day
costs like housekeeping and child care.
Benefit Reimbursement Amount
1st Day Hospital Confinement $500, once per year per insured member
Daily Hospital Confinement $100, up to 15 days per year, per insured member
Daily ICU Confinement $100, up to 15 days per year, per insured member
Additional Provisions
Coverage Type 24 hour
Covered Events Injury and Illness
Pregnancy Coverage Included
Pre-Existing Coverage 3 month look back period, 6 months treatment free, 12 month exclusion period
Portability Included
Monthly Rate
Employee Only $6.53
Employee Spouse $14.52
Employee Child(ren) $11.65
Employee Family $19.65
15