
Page 5 - 2022 Chartwell Hospitality - Non-Managers
P. 5
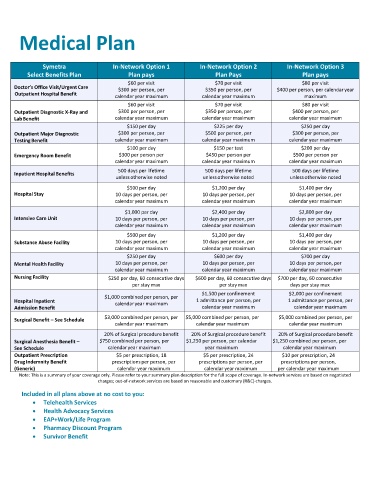
Medical Plan
Symetra In-Network Option 1 In-Network Option 2 In-Network Option 3
Select Benefits Plan Plan pays Plan Pays Plan pays
$60 per visit $70 per visit $80 per visit
Doctor’s Office Visit/Urgent Care $300 per person, per $350 per person, per $400 per person, per calendar year
Outpatient Hospital Benefit
calendar year maximum calendar year maximum maximum
$60 per visit $70 per visit $80 per visit
Outpatient Diagnostic X-Ray and $300 per person, per $350 per person, per $400 per person, per
Lab Benefit calendar year maximum calendar year maximum calendar year maximum
$150 per day $225 per day $250 per day
Outpatient Major Diagnostic $300 per person, per $500 per person, per $300 per person, per
Testing Benefit calendar year maximum calendar year maximum calendar year maximum
$100 per day $150 per test $200 per day
Emergency Room Benefit $300 per person per $450 per person per $500 per person per
calendar year maximum calendar year maximum calendar year maximum
500 days per lifetime 500 days per lifetime 500 days per lifetime
Inpatient Hospital Benefits
unless otherwise noted unless otherwise noted unless otherwise noted
$500 per day $1,200 per day $1,400 per day
Hospital Stay 10 days per person, per 10 days per person, per 10 days per person, per
calendar year maximum calendar year maximum calendar year maximum
$1,000 per day $2,400 per day $2,800 per day
Intensive Care Unit 10 days per person, per 10 days per person, per 10 days per person, per
calendar year maximum calendar year maximum calendar year maximum
$500 per day $1,200 per day $1,400 per day
Substance Abuse Facility 10 days per person, per 10 days per person, per 10 days per person, per
calendar year maximum calendar year maximum calendar year maximum
$250 per day $600 per day $700 per day
Mental Health Facility 10 days per person, per 10 days per person, per 10 days per person, per
calendar year maximum calendar year maximum calendar year maximum
Nursing Facility $250 per day, 60 consecutive days $600 per day, 60 consecutive days $700 per day, 60 consecutive
per stay max per stay max days per stay max
$1,500 per confinement $2,000 per confinement
$1,000 combined per person, per
Hospital Inpatient calendar year maximum 1 admittance per person, per 1 admittance per person, per
Admission Benefit calendar year maximum calendar year maximum
Surgical Benefit – See Schedule $3,000 combined per person, per $5,000 combined per person, per $5,000 combined per person, per
calendar year maximum
calendar year maximum calendar year maximum
20% of Surgical procedure benefit 20% of Surgical procedure benefit 20% of Surgical procedure benefit
Surgical Anesthesia Benefit – $750 combined per person, per $1,250 per person, per calendar $1,250 combined per person, per
See Schedule calendar year maximum year maximum calendar year maximum
Outpatient Prescription $5 per prescription, 18 $5 per prescription, 24 $10 per prescription, 24
Drug Indemnity Benefit prescriptions per person, per prescriptions per person, per prescriptions per person,
(Generic) calendar year maximum calendar year maximum per calendar year maximum
Note: This is a summary of your coverage only. Please refer to your summary plan description for the full scope of coverage. In-network services are based on negotiated
charges; out-of-network services are based on reasonable and customary (R&C) charges.
Included in all plans above at no cost to you:
• Telehealth Services
• Health Advocacy Services
• EAP+Work/Life Program
• Pharmacy Discount Program
• Survivor Benefit