
Page 12 - 2022 Penn Engineering Guide
P. 12
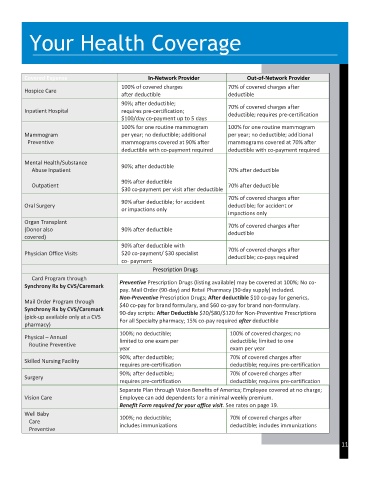
Your Health Coverage
Covered Expense In-Network Provider Out-of-Network Provider
100% of covered charges 70% of covered charges after
Hospice Care
after deductible deductible
90%; after deductible;
70% of covered charges after
Inpatient Hospital requires pre-certification;
deductible; requires pre-certification
$100/day co-payment up to 5 days
100% for one routine mammogram 100% for one routine mammogram
Mammogram per year; no deductible; additional per year; no deductible; additional
Preventive mammograms covered at 90% after mammograms covered at 70% after
deductible with co-payment required deductible with co-payment required
Mental Health/Substance
90%; after deductible
Abuse Inpatient 70% after deductible
90% after deductible
Outpatient 70% after deductible
$30 co-payment per visit after deductible
70% of covered charges after
90% after deductible; for accident
Oral Surgery deductible; for accident or
or impactions only
impactions only
Organ Transplant 70% of covered charges after
(Donor also 90% after deductible deductible
covered)
90% after deductible with
70% of covered charges after
Physician Office Visits $20 co-payment/ $30 specialist
deductible; co-pays required
co- payment
Prescription Drugs
Card Program through
Preventive Prescription Drugs (listing available) may be covered at 100%; No co-
Synchrony Rx by CVS/Caremark
pay. Mail Order (90-day) and Retail Pharmacy (30-day supply) included.
Non-Preventive Prescription Drugs; After deductible $10 co-pay for generics,
Mail Order Program through $40 co-pay for brand formulary, and $60 co-pay for brand non-formulary.
Synchrony Rx by CVS/Caremark
90-day scripts: After Deductible $20/$80/$120 for Non-Preventive Prescriptions
(pick-up available only at a CVS
For all Specialty pharmacy; 15% co-pay required after deductible
pharmacy)
100%; no deductible; 100% of covered charges; no
Physical – Annual limited to one exam per deductible; limited to one
Routine Preventive
year exam per year
90%; after deductible; 70% of covered charges after
Skilled Nursing Facility
requires pre-certification deductible; requires pre-certification
90%; after deductible; 70% of covered charges after
Surgery
requires pre-certification deductible; requires pre-certification
Separate Plan through Vision Benefits of America; Employee covered at no charge;
Vision Care Employee can add dependents for a minimal weekly premium.
Benefit Form required for your office visit. See rates on page 19.
Well Baby
100%; no deductible; 70% of covered charges after
Care
includes immunizations deductible; includes immunizations
Preventive
11