
Page 7 - Leona Arizona Employment Group Flipbook
P. 7
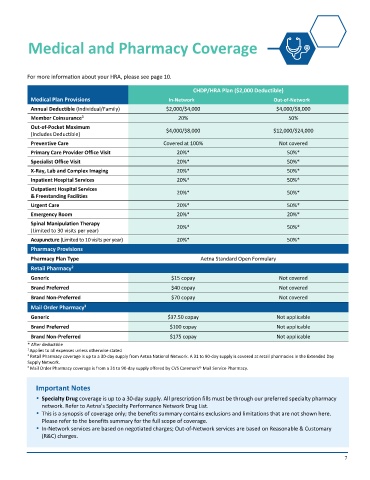
Medical and Pharmacy Coverage
For more information about your HRA, please see page 10.
CHDP/HRA Plan ($2,000 Deductible)
Medical Plan Provisions In-Network Out-of-Network
Annual Deductible (Individual/Family) $2,000/$4,000 $4,000/$8,000
1
Member Coinsurance 20% 50%
Out-of-Pocket Maximum $4,000/$8,000 $12,000/$24,000
(Includes Deductible)
Preventive Care Covered at 100% Not covered
Primary Care Provider Office Visit 20%* 50%*
Specialist Office Visit 20%* 50%*
X-Ray, Lab and Complex Imaging 20%* 50%*
Inpatient Hospital Services 20%* 50%*
Outpatient Hospital Services
& Freestanding Facilities 20%* 50%*
Urgent Care 20%* 50%*
Emergency Room 20%* 20%*
Spinal Manipulation Therapy 20%* 50%*
(Limited to 30 visits per year)
Acupuncture (Limited to 10 visits per year) 20%* 50%*
Pharmacy Provisions
Pharmacy Plan Type Aetna Standard Open Formulary
Retail Pharmacy
2
Generic $15 copay Not covered
Brand Preferred $40 copay Not covered
Brand Non-Preferred $70 copay Not covered
3
Mail Order Pharmacy
Generic $37.50 copay Not applicable
Brand Preferred $100 copay Not applicable
Brand Non-Preferred $175 copay Not applicable
* After deductible
1 Applies to all expenses unless otherwise stated
2 Retail Pharmacy coverage is up to a 30-day supply from Aetna National Network. A 31 to 90-day supply is covered at retail pharmacies in the Extended Day
Supply Network.
3 Mail Order Pharmacy coverage is from a 31 to 90-day supply offered by CVS Caremark® Mail Service Pharmacy.
Important Notes
Specialty Drug coverage is up to a 30-day supply. All prescription fills must be through our preferred specialty pharmacy
network. Refer to Aetna’s Specialty Performance Network Drug List.
This is a synopsis of coverage only; the benefits summary contains exclusions and limitations that are not shown here.
Please refer to the benefits summary for the full scope of coverage.
In-Network services are based on negotiated charges; Out-of-Network services are based on Reasonable & Customary
(R&C) charges.
7