
Page 10 - Emmis 2022 Benefit Guide
P. 10
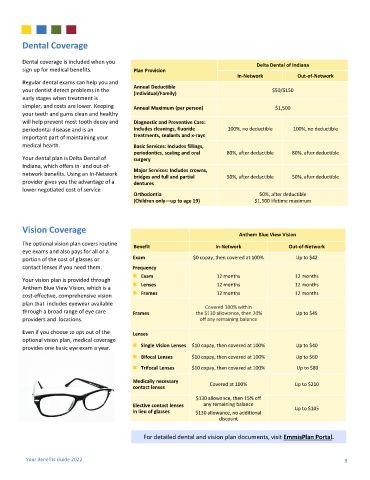
Dental Coverage
Dental coverage is included when you
Delta Dental of Indiana
sign up for medical benefits. Plan Provision
In-Network Out-of-Network
Regular dental exams can help you and
Annual Deductible
your dentist detect problems in the $50/$150
(Individual/Family)
early stages when treatment is
simpler, and costs are lower. Keeping Annual Maximum (per person) $1,500
your teeth and gums clean and healthy
will help prevent most tooth decay and Diagnostic and Preventive Care:
periodontal disease and is an Includes cleanings, fluoride 100%, no deductible 100%, no deductible
important part of maintaining your treatments, sealants and x-rays
medical health. Basic Services: Includes fillings,
periodontics, scaling and oral 80%, after deductible 80%, after deductible
Your dental plan is Delta Dental of surgery
Indiana, which offers in- and out-of-
Major Services: Includes crowns,
network benefits. Using an In-Network
bridges and full and partial 50%, after deductible 50%, after deductible
provider gives you the advantage of a dentures
lower negotiated cost of service
Orthodontia 50%, after deductible
(Children only—up to age 19) $1,500 lifetime maximum
Vision Coverage
Anthem Blue View Vision
The optional vision plan covers routine
Benefit In-Network Out-of-Network
eye exams and also pays for all or a
portion of the cost of glasses or Exam $0 copay, then covered at 100% Up to $42
contact lenses if you need them. Frequency
◼ Exam 12 months 12 months
Your vision plan is provided through
◼ Lenses 12 months 12 months
Anthem Blue View Vision, which is a
◼ Frames 12 months 12 months
cost-effective, comprehensive vision
plan that includes eyewear available
Covered 100% within
through a broad range of eye care Frames the $130 allowance, then 20% Up to $45
providers and locations. off any remaining balance
Even if you choose to opt out of the Lenses
optional vision plan, medical coverage
◼ Single Vision Lenses $10 copay, then covered at 100% Up to $40
provides one basic eye exam a year.
◼ Bifocal Lenses $10 copay, then covered at 100% Up to $60
◼ Trifocal Lenses $10 copay, then covered at 100% Up to $80
Medically necessary Covered at 100% Up to $210
contact lenses
$130 allowance, then 15% off
Elective contact lenses any remaining balance Up to $105
in lieu of glasses $130 allowance, no additional
discount
For detailed dental and vision plan documents, visit EmmisPlan Portal.
Your Benefits Guide 2022 9