
Page 2 - 2022 01 Inpats Murata FlipBook
P. 2
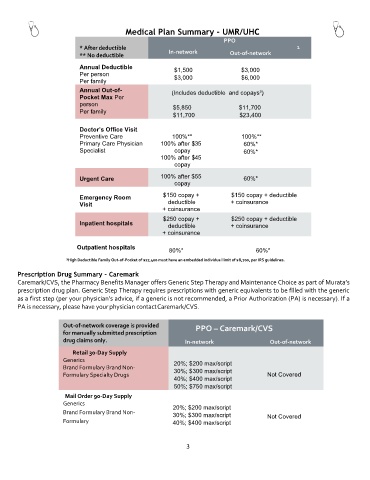
Medical Plan Summary – UMR/UHC
PPO
* After deductible In-network 1
** No deductible Out-of-network
Annual Deductible $1,500 $3,000
Per person
Per family $3,000 $6,000
Annual Out-of- (Includes deductible and copays²)
Pocket Max Per
person $5,850 $11,700
Per family
$11,700 $23,400
Doctor’s Office Visit
Preventive Care 100%** 100%**
Primary Care Physician 100% after $35 60%*
Specialist copay 60%*
100% after $45
copay
Urgent Care 100% after $55 60%*
copay
Emergency Room $150 copay + $150 copay + deductible
Visit deductible + coinsurance
+ coinsurance
$250 copay + $250 copay + deductible
Inpatient hospitals deductible + coinsurance
+ coinsurance
Outpatient hospitals
80%* 60%*
¹High Deductible Family Out-of-Pocket of $17,400 must have an embedded individual limit of $8,700, per IRS guidelines.
Prescription Drug Summary – Caremark
Caremark/CVS, the Pharmacy Benefits Manager offers Generic Step Therapy and Maintenance Choice as part of Murata’s
prescription drug plan. Generic Step Therapy requires prescriptions with generic equivalents to be filled with the generic
as a first step (per your physician’s advice, if a generic is not recommended, a Prior Authorization (PA) is necessary). If a
PA is necessary, please have your physician contact Caremark/CVS.
Out-of-network coverage is provided PPO – Caremark/CVS
for manually submitted prescription
drug claims only. In-network Out-of-network
Retail 30-Day Supply
Generics 20%; $200 max/script
Brand Formulary Brand Non- 30%; $300 max/script
Formulary Specialty Drugs Not Covered
40%; $400 max/script
50%; $750 max/script
Mail Order 90-Day Supply
Generics
20%; $200 max/script
Brand Formulary Brand Non-
30%; $300 max/script Not Covered
Formulary 40%; $400 max/script
3