
Page 3 - 2022 01 Inpats Murata FlipBook
P. 3
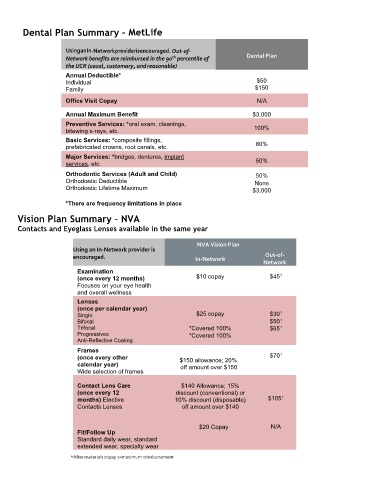
Dental Plan Summary – MetLife
Using an In- Network provider is encouraged. Out-of- Dental Plan
th
Network benefits are reimbursed in the 90 percentile of
the UCR (usual, customary, and reasonable)
Annual Deductible* $50
Individual
Family $150
Dental Plan
Office Visit Copay N/A
Annual Maximum Benefit $3,000
Preventive Services: *oral exam, cleanings, 100%
bitewing x-rays, etc.
Basic Services: *composite fillings,
prefabricated crowns, root canals, etc. 80%
Major Services: *bridges, dentures, implant 50%
services, etc.
Orthodontic Services (Adult and Child) 50%
Orthodontic Deductible None
Orthodontic Lifetime Maximum $3,000
*There are frequency limitations in place
Vision Plan Summary – NVA
Contacts and Eyeglass Lenses available in the same year
NVA Vision Plan
Using an In-Network provider is
encouraged. In-Network Out-of-
Network
Examination
1
(once every 12 months) $10 copay $45
Focuses on your eye health
and overall wellness
Lenses
(once per calendar year)
1
Single $25 copay $30
1
Bifocal $50
1
Trifocal *Covered 100% $65
Progressives *Covered 100%
Anti-Reflective Coating
Frames
1
(once every other $150 allowance; 20% $70
calendar year) off amount over $150
Wide selection of frames
Contact Lens Care $140 Allowance; 15%
(once every 12 discount (conventional) or
1
months) Elective 10% discount (disposable) $105
Contacts Lenses off amount over $140
$20 Copay N/A
Fit/Follow Up
Standard daily wear, standard
extended wear, specialty wear 6
*After materials copay 1=maximum reimbursement