
Page 7 - P4403.59-V46_Numark Magazine Feb 24- (1)
P. 7
FOR HEALTHCARE
PROFESSIONALS ONLY
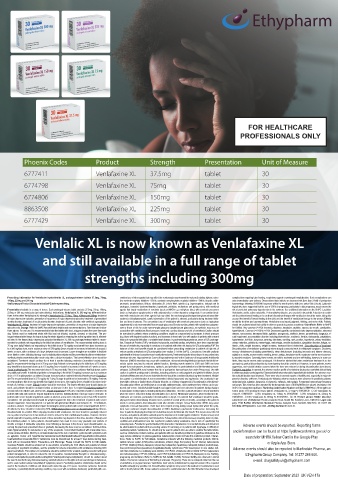
Phoenix Codes Product Strength Presentation Unit of Measure
6777411 Venlafaxine XL 37.5mg tablet 30
6774798 Venlafaxine XL 75mg tablet 30
6774806 Venlafaxine XL 150mg tablet 30
8863508 Venlafaxine XL 225mg tablet 30
6777429 Venlafaxine XL 300mg tablet 30
Venlalic XL is now known as Venlafaxine XL
and still available in a full range of tablet
strengths including 300mg
Prescribing Information for Venlafaxine hydrochloride XL prolonged-release tablets 37.5mg, 75mg, comitant use of other agents that may affect the serotonergic neurotransmitter system (including triptans, selec- complications requiring tube-feeding, respiratory support or prolonged hospitalisation. Such complications can
150mg, 225mg and 300 mg tive serotonin reuptake inhibitors - SSRIs, serotonin norepinephrine reuptake inhibitors - SNRIs, tricyclic antide- arise immediately upon delivery. Observational data indicate an increased risk (less than 2-fold) of postpartum
SeeSummaryofProductCharacteristics(SmPC)beforeprescribing. pressants, amphetamines, lithium, sibutramine,St. John’s Wort, opioids (e.g. buprenorphine, fentanyl and its haemorrhage following SSRI/SNRI exposure within the month prior to birth (see under Side Effects). Epidemio-
analogues, tramadol, dextromethorphan, tapentadol, pethidine, methadone and pentazocine), with medicinal logical data have suggested that the use of SSRIs in pregnancy, particularly in late pregnancy, may increase the
Presentation:Available in a range of doses. Each prolonged-release tablet contains 37.5mg, 75mg, 150mg, agents that impair metabolism of serotonin (such as MAOIs e.g. methylene blue), with serotonin precursors risk of persistent pulmonary hypertension in the newborn. See additional information on the SmPC. Lactation:
225mg or 300 mg venlafaxine (as hydrochloride). Indications: Venlafaxine XL 300 mg has differentindica- (such as tryptophan supplements) or with antipsychotics or other dopamine antagonists. If concomitant treat- Venlafaxine and its active metabolite, O-desmethylvenlafaxine, are excreted in breastmilk. A decision to contin-
tions to the other Venlafaxine XL strengths.Venlafaxine XL 37.5mg, 75mg, 150mg and 225mg: treatment ment with venlafaxine and other agents that may affect the serotonergicand/ordopaminergicneurotransmitter- ue/ discontinue breast feeding or to continue/ discontinue therapy with venlafaxine should be made, taking into
of major depressive episodes; prevention of recurrence of major depressive episodes; treatment of generalised systemsis clinicallywarranted, careful observation of the patient is advised, particularly during treatment initia- account the benefit of breast feeding to the child and the benefit of venlafaxine therapy to the woman. Effects
anxiety disorder; treatment of social anxiety disorder; treatment of panic disorder, with orwithout agoraphobia. tion and dose increases. The concomitant use of venlafaxine with serotonin precursors (such as tryptophan on ability to drive and use machines: Venlafaxine may impair judgment, thinking, and motor skills. Patients
Venlafaxine XL 300mg: treatment of major depressive episodes; prevention of recurrence of major depressive supplements) is not recommended.Narrow-angle glaucoma:Closely monitor patients with raisedintraocularpres- should be cautioned about their ability to drive or operate hazardous machinery. Side effects: Refer to SmPC
episodes only. Dosage: Refer to SmPC for additional details and recommendations. See licensed indica- sure or those at risk for acute narrow-angle glaucoma (angle-closure glaucoma), as mydriasis may occur in for full list. Very common (≥1/10): Insomnia, dizziness, headache, sedation, nausea, dry mouth, constipation,
tions above. For oral use. It is recommended to take the tablets with food, at approximately the same time each association with venlafaxine.Blood pressure, heart rate, cardiac disease and risk of arrhythmia:Caution should hyperhidrosis. Common (≥1/100 to <1/10): Decreased appetite, confusional state, depersonalization, abnormal
day. Tablets must be swallowed whole with fluid and not divided, crushed, chewed, or dissolved. The pro- be exercised in patients whose underlying conditions might be compromised by increases in blood pressure dreams, nervousness, decreased libido, agitation, anorgasmia, akathisia, tremor, paraesthesia, dysgeusia, vi-
longed-release tablet keeps its shape during the whole digestion releasing the active ingredient and is eliminat- (e.g. those with impaired cardiac function), and increases in heart rate. Use with caution in patients with a recent sual impairment, accomodation disorder including blurredvision, mydriasis, tinnitus, tachycardia, palpitations,
ed intact in the faeces.Major depressive episodes:Venlafaxine XL 300 mg prolonged-release tablet is recom- history of myocardial infarction or unstable heart disease. In postmarketing experience, cases of QTc prolonga- hypertension, hot flush, dyspnoea, yawning, diarrhoea, vomiting, rash, pruritus, hypertonia, urinary hesitation,
mended for patients not responding to the initial low doses of venlafaxine. The recommended starting dose is tion, Torsade de Pointes (TdP), ventricular tachycardia, and fatal cardiac arrhythmias have been reported with urinary retention, pollakiuria, menorrhagia, metorrhagia, erectile dysfunction, ejaculation disorder, fatigue, as-
75 mg once daily.Patients not responding to the initial dose of 75 mg/day may benefit from dose increases up the use of venlafaxine, especially in overdose or in patients with other risk factors for QTc prolongation/TdP.The thenia, chills, weight decrease, weight increase, increased blood cholesterol. Discontinuation of treatment:
to a 300 mg/day dose, and a maximum dose of 375mg/day.Doses should be increased at intervals of around 2 balance of risks and benefits should be considered before prescribing venlafaxine to patients at high risk of Discontinuation of venlafaxine (particularly when abrupt) commonly leads to withdrawal symptoms. Dizziness,
weeks or more, with a minimum of 4 days between each increment. Lower strengths are available to facilitate serious cardiac arrhythmia or QTc prolongation (see section 5.1 of the SmPC). Convulsions: Use with cautionin sensory disturbances (including paraethesia), sleep disturbances (including insomnia and intense dreams),
dose titration when initiating therapy and forindividualdoseadjustment.Becauseoftheriskofdose-relatedadver- patientswith a historyof convulsionsand monitorthemclosely.Treatmentshouldbe discontinued in any patient who agitation or anxiety, nausea and/or vomiting, tremor, vertigo, headache and flu syndrome are the most common-
seeffects,doseincrementsshouldbe made only after a clinical evaluation. The lowest effective dose should be develops seizures. Hyponatraemia: Cases of hyponatraemia and/ or the Syndrome of Inappropriate Antidiuretic ly reported reactions. Generally, these events are mild to moderate and are self-limiting; however, in some pa-
maintained. Treatment should continue for at least 6 months following remission.Generalised anxiety disor- Hormone (SIADH) secretion may occur with venlafaxine. Abnormal bleeding:Medicinal products that inhibit se- tients, they may be severe and/or prolonged. It is therefore advised that when venlafaxine treatment is no lon-
der:The recommended starting dose is 75 mg once daily.Patients not responding to the initial dose of 75 mg/day rotonin uptake may lead to reduced platelet function. Bleeding events related to SSRI and SNRI use have gerrequired, gradual discontinuation by dose tapering should be carried out. However, in some patients, severe
may benefit from increased doses up to 225 mg/day.Doses should be increased at intervals of 2 weeks or more. ranged from ecchymoses, hematomas, epistaxis, and petechiae to gastrointestinal and life-threatening haem- aggression, and suicidal ideation occurred when the dose was reduced or during discontinuation (see above).
Social anxietydisorder:The recommended dose is 75 mg once daily.There is no evidence that high doses confer orrhages. SSRIs/SNRIs may increase the risk of postpartum haemorrhage (see under Pregnancy). Use with Paediatric population: In general, the adverse reaction profile of venlafaxine (in placebo-controlled clinical trials)
any additional benefit. In individual patients not responding to the initial 75 mg/day, increases up to a maximum caution in patients predisposed to bleeding, including patients on anticoagulants and platelet inhibitors.Serum inchildrenandadolescents(ages6to17)wassimilartothatseenforadults.Inpaediatricclinicaltrials the adverse reac-
dose of 225 mg/daymaybe considered.Dosage increasescanbe madeat intervalsof2weeksormore.Panicdisor- cholesterol:Measurement of serum cholesterol levels should be considered during long-term treatment. Weight- tion suicidal ideation was observed. There were also increased reports of hostility and, especially in major de-
der:The recommended dose is 37.5 mg/day for 7 days.Dosage should then be increased to 75 mg/day. Patients loss agents: Co-administration is not recommended. Mania/ hypomania and aggression: Use cautiously in pa- pressive disorder, self-harm. Particularly, the following adverse reactions were observed in paediatric patients:
not responding to this dose may benefit from higher doses up to 225 mg/day.Doses should be increased at in- tients with a history or family history of bipolar disorder, or a history of aggression.Discontinuation of treatment:- abdominal pain, agitation, dyspepsia, ecchymosis, epistaxis, and myalgia. Postpartum haemorrhage frequency
tervals of 2 weeks or more. Elderly:Caution should be exercised. The lowest effective dose should always be Discontinuation effects are well known to occur with antidepressants, and sometimes these effects can be pro- not known: This event has been reported for the therapeutic class of SSRIs/SNRIs (see above). Overdose: See
used, and patients should be monitored when an increase in the dose is required.Paediatricpopulation:Not tracted and severe. Suicide/suicidal thoughts and aggression have been observed in patients during changes SmPC for management guidance. Marketing Authorisation Number and Basic NHS Price: All strengths are
recommended in children and adolescents. Hepatic impairment:A 50% dose reduction should be considered in in venlafaxine dosing regimen, including during discontinuation. Therefore, patients should be closely monitored sold in packs of 30 prolonged-release tablets. Venlafaxine XL 37.5mg PL 01883/0338 - £7.30; Venlafaxine XL
patients with mild and moderate hepatic impairment; however, individualisation of dosage may be desirable. In when the dose is reducedor during discontinuation (see above). Withdrawal symptoms, when treatment is dis- 75mg PL 01883/0339 – £2.60; Venlafaxine XL 150mg PL 01883/0340 - £3.90; Venlafaxine XL 225mg PL
patients with severe hepatic impairment caution is advised, and a dose reduction by more than 50% should be continued, are common, particularly if discontinuation is abrupt. It is advised that venlafaxine should be gradu- 01883/0341 - £33.60; Venlafaxine XL 300mg PL 01883/0363 - £37.50. Product Licence Holder: Macarthys
considered. The potential benefit should be weighed against the risk in the treatment of patients with severe ally tapered when discontinuing treatment over a period of several weeks or months, according to the patient’s Laboratories Ltd T/A Martindale Pharma, Bampton Road, Harold Hill, Romford, Essex, RM3 8UG. Legal cate-
hepatic impairment. Renal impairment: For patients with glomerular filtration rate between 30 – 70 ml/minute, needs. In some patients, discontinuation could take months or longer. Sexual dysfunction: SNRIs may cause gory: POM. Further information: Martindale Pharma, Bampton Road, Romford, RM3 8UG. Tel: 01277 266
caution is advised. For patients that require hemodialysis and in patients with severe renal impairment (GFR < symptoms of sexual dysfunction. There have been reports of long-lasting sexual dysfunction where the symp- 600. Date of Preparation: June 2023. Job Bag Number:UK-VEN-16.
30 ml/min, the dose should be reduced by 50%. Withdrawalsymptoms seen on discontinuation:Abrupt discon- toms have continued despite discontinuation of SNRI. Akathisia/ psychomotor restlessness: Increasing the
tinuationshould be avoided. When stopping treatment with venlafaxine, the dose should be gradually reduced dose in patients displaying development of akathisia may be detrimental. Dry mouth: This may increase the risk
over a period of at least one to two weeks in order to reduce the risk of withdrawal reactions. However, the time of caries, and patients should be advised upon the importance of dental hygiene.Diabetes: Treatment may need
period required for tapering and the amount of dose reduction may depend on the dose, duration of therapy and to be adjusted. Drug-Laboratory Test Interactions: False-positive urine immunoassay screening tests for phen-
the individual patient. In some patients, discontinuation may need to occur very gradually over periods of cyclidine and amphetamine have ben reported in patients taking venlafaxine, due to lack of specificityof the
months or longer. If intolerable symptoms occur following a decrease in the dose or upon discontinuation, re- screening tests. Potential for gastrointestinal (GI) obstruction: Venlafaxine XL is nondeformable and should not
suming the previously prescribed dose or gradually decreasing the dose may be considered. Contra-indica- be administered to patients with pre-existing severe GI narrowing or in patients with dysphagia or difficulty in Adverse events should be reported. Reporting forms
tions:Hypersensitivity to venlafaxine or any of the excipients. Concomitant treatment with irreversible mono- swallowing tablets. Venlafaxine XL should only be used in patients who are able to swallow the tablet whole. and information can be found at https://yellowcard.mhra.gov.uk/ or
amine oxidase inhibitors (MAOIs) is contraindicated due to the risk of serotonin syndrome with symptoms such Lactose: Venlafaxine contains lactose, and patients with rare hereditary problems of galactose intolerance, the
as agitation, tremor and hyperthermia.Venlafaxinemustnotbeinitiatedforatleast14daysafterdiscontinuationof- Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicinal product. Interac- search for MHRA Yellow Card in the Google Play
treatmentwithan irreversible MAOI. Venlafaxine must be discontinued for at least 7 days before starting treat- tions: Refer to SmPC for full details. Venlafaxine interacts with the following medicinal products: MAOIs;
ment with an irreversible MAOI. Precautions and Warnings: Please consult the SmPC for full details. central nervous system (CNS)-active substances; ethanol; drugs that prolong the QT interval; ketoconazole or Apple App Store.
Overdose:Patients should be advised not to use alcohol, considering its CNS effects and potential of clinical (CYP3A4 inhibitor); lithium; diazepam; imipramine; haloperidol; risperidone; metoprolol;indinavir;oralcontracep-
worsening of psychiatric conditions, and the potential for adverse interactions with venlafaxine including CNS tives;serotoninsyndrome(seeabove).DrugsMetabolizedby Cytochrome P450 Isoenzymes: In vivo studies indi- Adverse events should also be reported to Martindale Pharma, an
depressant effects. Prescriptions for venlafaxine should be written for the smallest quantity consistent with good cate that venlafaxine is a relatively weak inhibitor of CYP2D6. Venlafaxine did not inhibit CYP3A4 (alprazolam
patient management, in order to reduce the risk of overdose. Suicide/suicidal thoughts or clinicalworsening:- and carbamazepine), CYP1A2 (caffeine), and CYP2C9 (tolbutamide) or CYP2C19 (diazepam) in vivo. Fertility, Ethypharm Group Company. Tel: 01277 266 600.
Closelymonitorpatients,inparticularthoseathighrisk.Patients(andcaregiversofpatients) should be alerted about pregnancy and lactation: Refer to SmPC for full details. Fertility: Reduced fertility was observed in animal
the need to monitor for any clinical worsening, suicidal behaviour or thoughts and unusual changes in behaviour, studies. The human relevance of this finding is unknown. Pregnancy: There are no adequate data from the use e-mail: drugsafety.uk@ethypharm.com
and to seek medical advice immediately if symptoms present. Paediatricpopulation: Venlafaxine should not be of venlafaxine in pregnant women. Venlafaxine must only be administered to pregnant women if the expected
used in the treatment of children and adolescents under the age of 18 years. Serotonin syndrome: Serotonin benefits outweigh any possible risk. Discontinuation symptoms may occur in the newborns if venlafaxine is used
syndrome, a potentially life-threatening condition, may occur with venlafaxine treatment, particularly with con- until or shortly before birth. Some newborns exposed to venlafaxine late in the third trimester have developed
Date of preparation: September 2023 UK-VEN-17a
15/01/2024 14:38:20
P4403.59-V46_Numark Magazine Feb 24-.indd 7 15/01/2024 14:38:20
P4403.59-V46_Numark Magazine Feb 24-.indd 7