
Page 14 - 2021 Master's University Benefit Brochure_Final3
P. 14
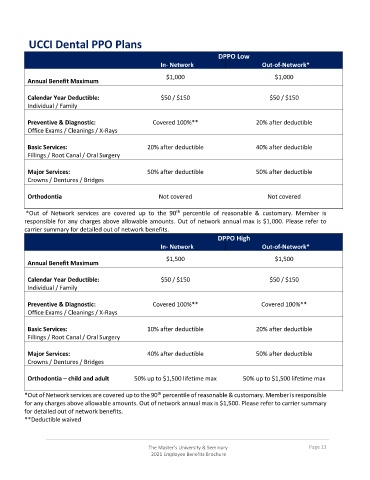
UCCI Dental PPO Plans
DPPO Low
In- Network Out-of-Network*
$1,000 $1,000
Annual Benefit Maximum
Calendar Year Deductible: $50 / $150 $50 / $150
Individual / Family
Preventive & Diagnostic: Covered 100%** 20% after deductible
Office Exams / Cleanings / X-Rays
Basic Services: 20% after deductible 40% after deductible
Fillings / Root Canal / Oral Surgery
Major Services: 50% after deductible 50% after deductible
Crowns / Dentures / Bridges
Orthodontia Not covered Not covered
th
*Out of Network services are covered up to the 90 percentile of reasonable & customary. Member is
responsible for any charges above allowable amounts. Out of network annual max is $1,000. Please refer to
carrier summary for detailed out of network benefits.
DPPO High
In- Network Out-of-Network*
$1,500 $1,500
Annual Benefit Maximum
Calendar Year Deductible: $50 / $150 $50 / $150
Individual / Family
Preventive & Diagnostic: Covered 100%** Covered 100%**
Office Exams / Cleanings / X-Rays
Basic Services: 10% after deductible 20% after deductible
Fillings / Root Canal / Oral Surgery
Major Services: 40% after deductible 50% after deductible
Crowns / Dentures / Bridges
Orthodontia – child and adult 50% up to $1,500 lifetime max 50% up to $1,500 lifetime max
th
*Out of Network services are covered up to the 90 percentile of reasonable & customary. Member is responsible
for any charges above allowable amounts. Out of network annual max is $1,500. Please refer to carrier summary
for detailed out of network benefits.
**Deductible waived
The Master’s University & Seminary Page 13
2021 Employee Benefits Brochure