
Page 8 - 2021 Master's University Benefit Brochure_Final3
P. 8
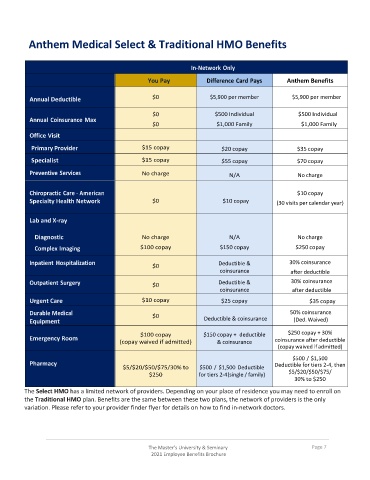
Anthem Medical Select & Traditional HMO Benefits
In-Network Only
You Pay Difference Card Pays Anthem Benefits
Annual Deductible $0 $5,900 per member $5,900 per member
$0 $500 Individual $500 Individual
Annual Coinsurance Max
$0 $1,000 Family $1,000 Family
Office Visit
Primary Provider $15 copay $20 copay $35 copay
Specialist $15 copay $55 copay $70 copay
Preventive Services No charge N/A No charge
Chiropractic Care - American $10 copay
Specialty Health Network $0 $10 copay (30 visits per calendar year)
Lab and X-ray
Diagnostic No charge N/A No charge
Complex Imaging $100 copay $150 copay $250 copay
Inpatient Hospitalization Deductible & 30% coinsurance
$0
coinsurance after deductible
Outpatient Surgery $0 Deductible & 30% coinsurance
coinsurance after deductible
Urgent Care $10 copay $25 copay $35 copay
Durable Medical 50% coinsurance
$0
Equipment Deductible & coinsurance (Ded. Waived)
$100 copay $150 copay + deductible $250 copay + 30%
Emergency Room coinsurance after deductible
(copay waived if admitted) & coinsurance
(copay waived if admitted)
$500 / $1,500
Pharmacy Deductible for tiers 2-4, then
$5/$20/$50/$75/30% to $500 / $1,500 Deductible
$250 for tiers 2-4 (single / family) $5/$20/$50/$75/
30% to $250
The Select HMO has a limited network of providers. Depending on your place of residence you may need to enroll on
the Traditional HMO plan. Benefits are the same between these two plans, the network of providers is the only
variation. Please refer to your provider finder flyer for details on how to find in-network doctors.
The Master’s University & Seminary Page 7
2021 Employee Benefits Brochure