
Page 10 - RTF.20 Employee Benefits
P. 10
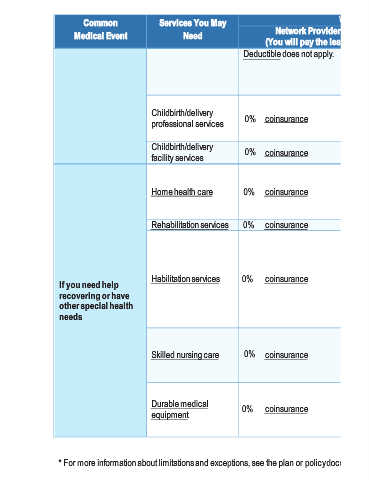
Network Provider What You Will Pay Exceptions, & Limitations, Out-of-Network Provider Other Important Information (You will pay the most) (You will pay the least) Maternity care may include tests Deductible does not apply. and services described elsewhere in the SBC (i.e. ultrasound). Prior Authorization is required for inpatient services. If you don't get Prior Authorization, coinsurance coinsurance 50% benefits could be reduced by 50
Services You May Need Childbirth/delivery 0% professional services Childbirth/delivery 0% facility services 0% Home health care 0% Rehabilitation services 0% Habilitation services 0% Skilled nursing care Durable medical 0% equipment
Common Medical Event If you need help recovering or have other special health needs