
Page 13 - RTF.20 Employee Benefits
P. 13
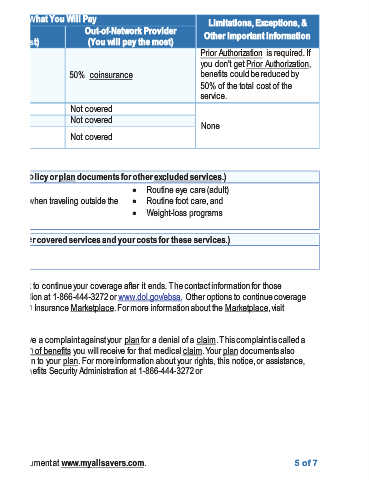
Exceptions, & Other Important Information is required. If 5of 7
Limitations, Prior Authorization you don't get Prior Authorization, benefits could be reduced by 50% of the total cost of the service. None Routine eye care (adult) Routine foot care, and Weight-loss programs
Out-of-Network Provider (You will pay the most) coinsurance x x x
What You Will Pay 50% Not covered Not covered Not covered Non-emergency care when traveling outside the
Network Provider (You will pay the least) coinsurance Not covered Not covered Not covered Does NOT Cover (This isn’t a complete list. Check your policy or plan documentsforotherexcluded services.) Long-term care x x United States Private-duty nursing x Other Covered Services (This isn’t a complete list.Check your policy for other covered services and your costs for these services.) Hearing aids x Your Rights to Continue Coverage:There are a
Services You May Need 0% Hospice services Children’s eye exam Children’s glasses Children’s dental check- up Does this plan provide Minimum Essential Coverage? Yes.
Common Medical Event If your child needs dental or eye care Excluded Services & Other Covered Services: Services Your Plan Bariatric surgery x Cosmetic surgery x Dental care (adult) x Infertility treatment x Acupuncture x Chiropractic care, and x www.HealthCare.gov or call 1-800-318-2596. www.dol.gov/ebsa/healthreform.