
Page 156 - YORAM RUDY BOOK FINAL
P. 156
P. 156
5.7 Arrhythmic Substrates of Hereditary Cardiac Disorders
The Long QT (LQT) Syndrome 309
The congenital LQT syndrome is an inherited cardiac channelopathy that can cause
syncope and sudden death in young adults with structurally normal hearts . Arrhythmias in
310
these patients are classified as polymorphic ventricular tachycardia (torsades de pointes).
The genetic and molecular basis of LQT has been studied extensively 311,312 . However, the arrhythmic
substrate in the hearts of LQT patients has not been fully defined. We have used ECGI to map the
EP substrate in 25 patients with genotype-positive, phenotype-positive LQT syndrome 309 . Based
on identified mutations there were nine LQT1 patients (loss-of-function mutations in KCNQ1,
leading to reduced I ), nine LQT2 (loss-of-function mutations in KCNH2 and reduced I ), five LQT3
Kr
Ks
(gain-of-function mutations in SCN5A and increased I ) and two LQT5 (loss- of-function
Na
mutations in KCNE1 and reduced I ). Epicardial activation in sinus rhythm is normal in all LQT
Ks
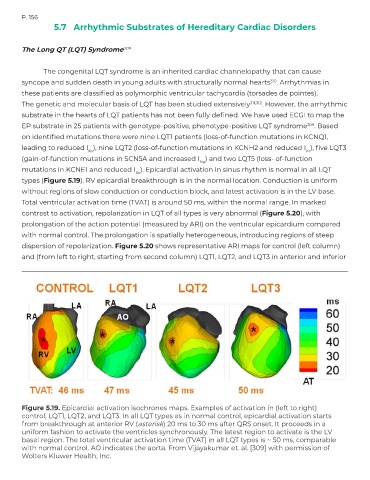
types (Figure 5.19). RV epicardial breakthrough is in the normal location. Conduction is uniform
without regions of slow conduction or conduction block, and latest activation is in the LV base.
Total ventricular activation time (TVAT) is around 50 ms, within the normal range. In marked
contrast to activation, repolarization in LQT of all types is very abnormal (Figure 5.20), with
prolongation of the action potential (measured by ARI) on the ventricular epicardium compared
with normal control. The prolongation is spatially heterogeneous, introducing regions of steep
dispersion of repolarization. Figure 5.20 shows representative ARI maps for control (left column)
and (from left to right, starting from second column) LQT1, LQT2, and LQT3 in anterior and inferior
Figure 5.19. Epicardial activation isochrones maps. Examples of activation in (left to right)
control, LQT1, LQT2, and LQT3. In all LQT types as in normal control, epicardial activation starts
from breakthrough at anterior RV (asterisk) 20 ms to 30 ms after QRS onset. It proceeds in a
uniform fashion to activate the ventricles synchronously. The latest region to activate is the LV
basal region. The total ventricular activation time (TVAT) in all LQT types is ~ 50 ms, comparable
with normal control. AO indicates the aorta. From Vijayakumar et. al. [309] with permission of
Wolters Kluwer Health, Inc.