
Page 157 - YORAM RUDY BOOK FINAL
P. 157
P. 157
views. For example, maximum ARI in LQT3 is 430 ms compared to only 320 ms in control.
The regional, heterogeneous prolongation of ARI introduces sharp repolarization gradients in all
LQT types (indicated by black arrows in Figure 5.20). Mean ARI gradient is 92±18 ms/cm in LQT1,
117±29 ms/cm in LQT2, and 129±4 ms/cm in LQT3, compared to only 2.0±2.0 ms/cm in control.
The presence of steep repolarization dispersion creates conditions for the development of
unidirectional block and reentrant arrhythmias. Interestingly, the magnitude and location of steep
repolarization gradients varies among patients, even with the same genetic mutation. However,
repolarization gradients were significantly steeper (130±27 ms/cm) in symptomatic compared to
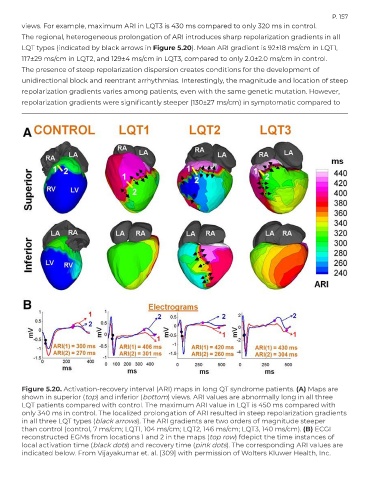
Figure 5.20. Activation-recovery interval (ARI) maps in long QT syndrome patients. (A) Maps are
shown in superior (top) and inferior (bottom) views. ARI values are abnormally long in all three
LQT patients compared with control. The maximum ARI value in LQT is 450 ms compared with
only 340 ms in control. The localized prolongation of ARI resulted in steep repolarization gradients
in all three LQT types (black arrows). The ARI gradients are two orders of magnitude steeper
than control (control, 7 ms/cm; LQT1, 104 ms/cm; LQT2, 146 ms/cm; LQT3, 140 ms/cm). (B) ECGI
reconstructed EGMs from locations 1 and 2 in the maps (top row) fdepict the time instances of
local activation time (black dots) and recovery time (pink dots). The corresponding ARI values are
indicated below. From Vijayakumar et. al. [309] with permission of Wolters Kluwer Health, Inc.