
Page 173 - Modul English Communication In Nursing
P. 173
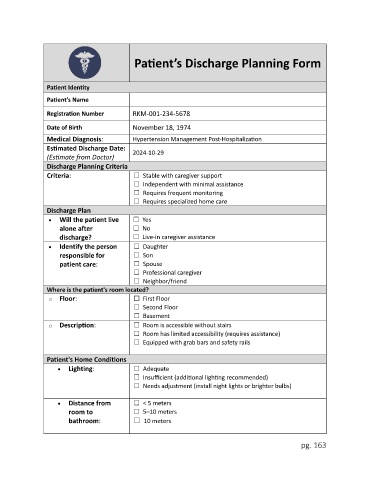
Patient’s Discharge Planning Form
Patient Identity
Patient’s Name
Registration Number RKM-001-234-5678
Date of Birth November 18, 1974
Medical Diagnosis: Hypertension Management Post-Hospitalization
Estimated Discharge Date:
2024-10-29
(Estimate from Doctor)
Discharge Planning Criteria
Criteria: ☐ Stable with caregiver support
☐ Independent with minimal assistance
☐ Requires frequent monitoring
☐ Requires specialized home care
Discharge Plan
• Will the patient live ☐ Yes
alone after ☐ No
discharge? ☐ Live-in caregiver assistance
• Identify the person ☐ Daughter
responsible for ☐ Son
patient care: ☐ Spouse
☐ Professional caregiver
☐ Neighbor/friend
Where is the patient's room located?
o Floor: ☐ First Floor
☐ Second Floor
☐ Basement
o Description: ☐ Room is accessible without stairs
☐ Room has limited accessibility (requires assistance)
☐ Equipped with grab bars and safety rails
Patient's Home Conditions
• Lighting: ☐ Adequate
☐ Insufficient (additional lighting recommended)
☐ Needs adjustment (install night lights or brighter bulbs)
• Distance from ☐ < 5 meters
room to ☐ 5–10 meters
bathroom: ☐ 10 meters
pg. 163