
Page 91 - Rapid Review of ECG Interpretation in Small Animal Practice, 2nd Edition
P. 91
Answer 26 ECG Cases
Answer 26
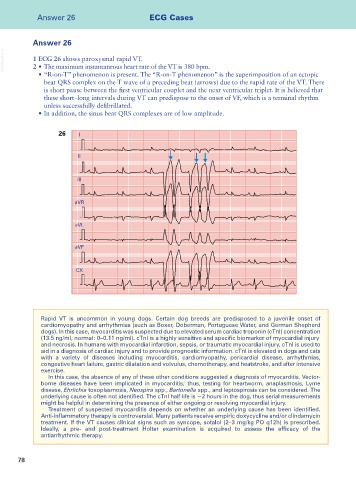
VetBooks.ir 1 ECG 26 shows paroxysmal rapid VT.
2 • The maximum instantaneous heart rate of the VT is 380 bpm.
• “R-on-T” phenomenon is present. The “R-on-T phenomenon” is the superimposition of an ectopic
beat QRS complex on the T wave of a preceding beat (arrows) due to the rapid rate of the VT. There
is short pause between the first ventricular couplet and the next ventricular triplet. It is believed that
these short–long intervals during VT can predispose to the onset of VF, which is a terminal rhythm
unless successfully defibrillated.
• In addition, the sinus beat QRS complexes are of low amplitude.
26 I
II
III
aVR
aVL
aVF
CX
Rapid VT is uncommon in young dogs. Certain dog breeds are predisposed to a juvenile onset of
cardiomyopathy and arrhythmias (such as Boxer, Doberman, Portuguese Water, and German Shepherd
dogs). In this case, myocarditis was suspected due to elevated serum cardiac troponin (cTnI) concentration
(13.5 ng/ml, normal: 0–0.11 ng/ml). cTnI is a highly sensitive and specific biomarker of myocardial injury
and necrosis. In humans with myocardial infarction, sepsis, or traumatic myocardial injury, cTnI is used to
aid in a diagnosis of cardiac injury and to provide prognostic information. cTnI is elevated in dogs and cats
with a variety of diseases including myocarditis, cardiomyopathy, pericardial disease, arrhythmias,
congestive heart failure, gastric dilatation and volvulus, chemotherapy, and heatstroke, and after intensive
exercise.
In this case, the absence of any of these other conditions suggested a diagnosis of myocarditis. Vector-
borne diseases have been implicated in myocarditis; thus, testing for heartworm, anaplasmosis, Lyme
disease, Ehrlichia toxoplasmosis, Neospira spp., Bartonella spp., and leptospirosis can be considered. The
underlying cause is often not identified. The cTnI half-life is ~2 hours in the dog, thus serial measurements
might be helpful in determining the presence of either ongoing or resolving myocardial injury.
Treatment of suspected myocarditis depends on whether an underlying cause has been identified.
Anti-inflammatory therapy is controversial. Many patients receive empiric doxycycline and/or clindamycin
treatment. If the VT causes clinical signs such as syncope, sotalol (2–3 mg/kg PO q12h) is prescribed.
Ideally, a pre- and post-treatment Holter examination is acquired to assess the efficacy of the
antiarrhythmic therapy.
78