
Page 106 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 106
96 ELECTROLYTE DISORDERS
reabsorption and secretion are made. Potassium gradient for potassium reabsorption via the paracellular
experiences either net reabsorption or secretion in the route. Transcellular reabsorption of potassium is
þ
þ
connecting tubule, cortical collecting duct, and first por- facilitated by the luminal Na -K -2Cl cotransporter
þ
tion of the outer medullary collecting duct, depending on and by potassium channels and a K -Cl cotransporter
the body’s needs. Net movement of potassium in these in the basolateral membranes (Fig. 5-6).
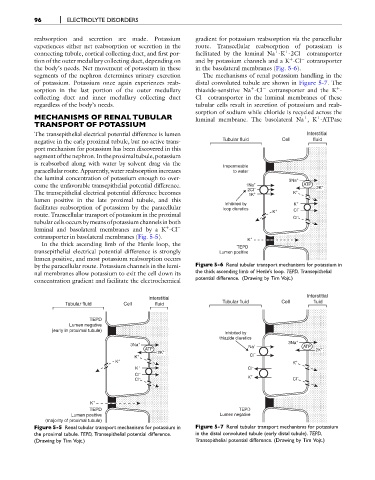
segments of the nephron determines urinary excretion The mechanisms of renal potassium handling in the
of potassium. Potassium once again experiences reab- distal convoluted tubule are shown in Figure 5-7. The
þ
þ
sorption in the last portion of the outer medullary thiazide-sensitive Na -Cl cotransporter and the K -
collecting duct and inner medullary collecting duct Cl cotransporter in the luminal membranes of these
regardless of the body’s needs. tubular cells result in secretion of potassium and reab-
sorption of sodium while chloride is recycled across the
MECHANISMS OF RENAL TUBULAR luminal membrane. The basolateral Na ,K -ATPase
þ
þ
TRANSPORT OF POTASSIUM
The transepithelial electrical potential difference is lumen Interstitial
negative in the early proximal tubule, but no active trans- Tubular fluid Cell fluid
port mechanism for potassium has been discovered in this
segment ofthe nephron. In the proximal tubule, potassium
is reabsorbed along with water by solvent drag via the
Impermeable
paracellular route. Apparently, water reabsorption increases to water
the luminal concentration of potassium enough to over- 3Na +
come the unfavorable transepithelial potential difference. 1Na + ATP 2K +
2Cl –
The transepithelial electrical potential difference becomes 1K + K +
lumen positive in the late proximal tubule, and this
Inhibited by K +
facilitates reabsorption of potassium by the paracellular loop diuretics + Cl –
route. Transcellular transport of potassium in the proximal K
Cl –
tubular cells occurs by meansofpotassiumchannels inboth
luminal and basolateral membranes and by a K -Cl
þ
cotransporter in basolateral membranes (Fig. 5-5). +
K
In the thick ascending limb of the Henle loop, the
TEPD
transepithelial electrical potential difference is strongly Lumen positive
lumen positive, and most potassium reabsorption occurs
by the paracellular route. Potassium channels in the lumi- Figure 5-6 Renal tubular transport mechanisms for potassium in
nal membranes allow potassium to exit the cell down its the thick ascending limb of Henle’s loop. TEPD, Transepithelial
potential difference. (Drawing by Tim Vojt.)
concentration gradient and facilitate the electrochemical
Interstitial
Interstitial
Tubular fluid Cell fluid Tubular fluid Cell fluid
TEPD
Lumen negative
(early in proximal tubule)
Inhibited by
thiazide diuretics
3Na + Na + 3Na + ATP
ATP 2K +
2K + –
K + Cl
K + K +
K + Cl –
Cl – K +
Cl – Cl –
K +
TEPD TEPD
Lumen positive Lumen negative
(majority of proximal tubule)
Figure 5-5 Renal tubular transport mechanisms for potassium in Figure 5-7 Renal tubular transport mechanisms for potassium
the proximal tubule. TEPD, Transepithelial potential difference. in the distal convoluted tubule (early distal tubule). TEPD,
(Drawing by Tim Vojt.) Transepithelial potential difference. (Drawing by Tim Vojt.)