
Page 281 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 281
272 ACID-BASE DISORDERS
the alkalosis. Hypokalemia also stimulates renal HCO 3 – Mechanism
ammoniagenesis, presumably through stimulation of glu- Alkali load Cl + – of buffering
taminase via decreased pH i . The increase in renal ammo- 2% lac H
nium excretion enhances renal acid excretion and 4% lac –
contributes to increased plasma HCO 3 concentration. Na , K +
+
Hypokalemia also may decrease the GFR as a conse- 26% Pr H +
Pi
32%
quence of glomerular hemodynamic changes and may Pr – Intracellular
directly impair chloride reabsorption in the distal neph- Pi –
buffering
ron, resulting in enhanced lumen electronegativity and
þ
facilitation of H secretion into tubular fluid.
RESPONSE OF THE BODY TO
METABOLIC ALKALOSIS
The body’s response to metabolic alkalosis is the reverse
of its response to administration of a mineral acid such as 67% HCO 3 –
HCl. The kidneys are more effective in excreting an alka- retained in ECF
line load than an acid load, provided that the subject is 68%
Extracellular
not sodium avid and sufficient chloride is provided.
buffering
Acute Buffer Response
In an early study of the buffer response to alkali, HPr → H + Pr –
+
1%
+
–
nephrectomized dogs were given 20 mEq/kg NaHCO 3 H + HCO 3 → H 2 CO 3 → H 2 O + ↑CO 2
with a resultant increase in plasma HCO 3 concentration
to approximately 60 mEq/L. 222 Of the administered Metabolic alkalosis
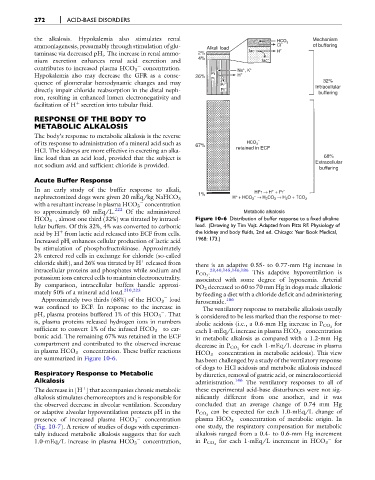
HCO 3 , almost one third (32%) was titrated by intracel- Figure 10-6 Distribution of buffer response to a fixed alkaline
lular buffers. Of this 32%, 4% was converted to carbonic load. (Drawing by Tim Vojt. Adapted from Pitts RF. Physiology of
acid by H from lactic acid released into ECF from cells. the kidney and body fluids, 2nd ed. Chicago: Year Book Medical,
þ
Increased pH i enhances cellular production of lactic acid 1968: 173.)
by stimulation of phosphofructokinase. Approximately
2% entered red cells in exchange for chloride (so-called
þ
chloride shift), and 26% was titrated by H released from there is an adaptive 0.55- to 0.77-mm Hg increase in
intracellular proteins and phosphates while sodium and . 23,40,145,146,186 This adaptive hypoventilation is
potassium ions entered cells to maintain electroneutrality. P CO 2
associated with some degree of hypoxemia. Arterial
By comparison, intracellular buffers handle approxi- PO 2 decreased to 60 to 70 mm Hg in dogs made alkalotic
mately 50% of a mineral acid load. 210,223 by feeding a diet with a chloride deficit and administering
Approximately two thirds (68%) of the HCO 3 load furosemide. 186
was confined to ECF. In response to the increase in The ventilatory response to metabolic alkalosis usually
pH, plasma proteins buffered 1% of this HCO 3 . That is considered to be less marked than the response to met-
is, plasma proteins released hydrogen ions in numbers for
abolic acidosis (i.e., a 0.6-mm Hg increase in P CO 2
sufficient to convert 1% of the infused HCO 3 to car- each 1-mEq/L increase in plasma HCO 3 concentration
bonic acid. The remaining 67% was retained in the ECF in metabolic alkalosis as compared with a 1.2-mm Hg
compartment and contributed to the observed increase for each 1-mEq/L decrease in plasma
decrease in P CO 2
in plasma HCO 3 concentration. These buffer reactions HCO 3 concentration in metabolic acidosis). This view
are summarized in Figure 10-6. has been challenged by a study of the ventilatory response
of dogs to HCl acidosis and metabolic alkalosis induced
Respiratory Response to Metabolic by diuretics, removal of gastric acid, or mineralocorticoid
Alkalosis administration. 146 The ventilatory responses to all of
The decrease in [H ] that accompanies chronic metabolic these experimental acid-base disturbances were not sig-
þ
alkalosis stimulates chemoreceptors and is responsible for nificantly different from one another, and it was
the observed decrease in alveolar ventilation. Secondary concluded that an average change of 0.74 mm Hg
or adaptive alveolar hypoventilation protects pH in the P CO 2 can be expected for each 1.0-mEq/L change of
concentration of metabolic origin. In
presence of increased plasma HCO 3 concentration plasma HCO 3
(Fig. 10-7). A review of studies of dogs with experimen- one study, the respiratory compensation for metabolic
tally induced metabolic alkalosis suggests that for each alkalosis ranged from a 0.4- to 0.6-mm Hg increment
for
1.0-mEq/L increase in plasma HCO 3 concentration, in P CO 2 for each 1-mEq/L increment in HCO 3