
Page 286 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 286
Metabolic Acid-Base Disorders 277
Extracellular Gastric Lumen allows retained HCO 3 to be excreted in the urine. Urine
fluid parietal cell of stomach pH increases as HCO 3 is excreted, indicating a favorable
response to therapy. Chloride once again appears in the
CO + H O
2
2
urine whenthe alkalosisisresolved.Thecritical factor inres-
CO
H 2 3 olution of this form of alkalosis is the provision of chloride as a
–
HCO 3 – HCO + H + H + resorbable anion. Alkalosis can be corrected without provi-
3
sion of sodium or potassium as long as chloride is provided.
Cl – Cl – Clinically, however, alkalosis is corrected by administering
some combination of NaCl and KCl.
Pancreatic Lumen Diuretic Administration
duct cell of duodenum
Diuretics cause approximately equal losses of sodium and
CO + H O chloride in the urine, but the concentration of chloride in
2
2
ECF is less than that of sodium by approximately
H CO 3
2
35 mEq/L. Thus, these drugs may cause chloride-
H + H + HCO 3 – HCO 3 – responsive metabolic alkalosis by a disproportionate loss
+
of chloride in urine and creation of a relative chloride def-
Na + Na +
icit in ECF. Increased renal sodium avidity is also an
important factor in development of the metabolic alkalo-
sis and potassium depletion that may occur during
Ileal or colonic Lumen diuretic administration.
epithelial cell of ileum Loop diuretics inhibit NaCl reabsorption in the thick
or colon
ascending limb of Henle’s loop by competing with chlo-
þ
þ
ride for the Na -K -2Cl luminal carrier. This causes
Na + Na + increased delivery of sodium to the distal nephron, where
þ
þ
þ
accelerated Na -H and Na -K exchange occurs as the
þ
Cl – Cl –
kidneys attempt to retain more sodium. Increased reli-
ance of the kidneys on these mechanisms for sodium reab-
sorption contributes to metabolic alkalosis and potassium
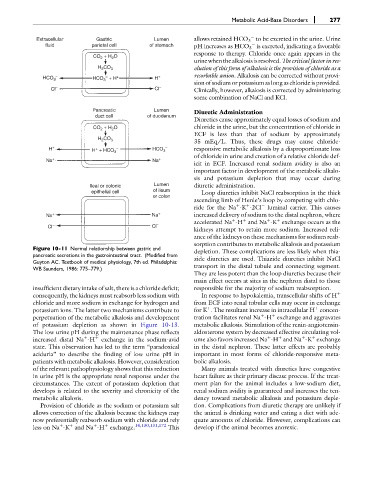
Figure 10-11 Normal relationship between gastric and
pancreatic secretions in the gastrointestinal tract. (Modified from depletion. These complications are less likely when thia-
Guyton AC. Textbook of medical physiology, 7th ed. Philadelphia: zide diuretics are used. Thiazide diuretics inhibit NaCl
WB Saunders, 1986: 775–779.) transport in the distal tubule and connecting segment.
They are less potent than the loop diuretics because their
main effect occurs at sites in the nephron distal to those
insufficient dietary intake of salt, there is a chloride deficit; responsible for the majority of sodium reabsorption.
consequently, the kidneys must reabsorb less sodium with In response to hypokalemia, transcellular shifts of H þ
chloride and more sodium in exchange for hydrogen and from ECF into renal tubular cells may occur in exchange
þ
þ
potassium ions. The latter two mechanisms contribute to for K . The resultant increase in intracellular H concen-
þ
þ
perpetuation of the metabolic alkalosis and development tration facilitates renal Na -H exchange and aggravates
of potassium depletion as shown in Figure 10-13. metabolic alkalosis. Stimulation of the renin-angiotensin-
The low urine pH during the maintenance phase reflects aldosterone system by decreased effective circulating vol-
þ
þ
þ
þ
þ
increased distal Na -H þ exchange in the sodium-avid ume also favors increased Na -H and Na -K exchange
state. This observation has led to the term “paradoxical in the distal nephron. These latter effects are probably
aciduria” to describe the finding of low urine pH in important in most forms of chloride-responsive meta-
patients with metabolic alkalosis. However, consideration bolic alkalosis.
of the relevant pathophysiology shows that this reduction Many animals treated with diuretics have congestive
in urine pH is the appropriate renal response under the heart failure as their primary disease process. If the treat-
circumstances. The extent of potassium depletion that ment plan for the animal includes a low-sodium diet,
develops is related to the severity and chronicity of the renal sodium avidity is guaranteed and increases the ten-
metabolic alkalosis. dency toward metabolic alkalosis and potassium deple-
Provision of chloride as the sodium or potassium salt tion. Complications from diuretic therapy are unlikely if
allows correction of the alkalosis because the kidneys may the animal is drinking water and eating a diet with ade-
now preferentially reabsorb sodium with chloride and rely quate amounts of chloride. However, complications can
þ
þ
þ
less on Na -K and Na -H exchange. 14,130,131,172 This develop if the animal becomes anorexic.
þ