
Page 223 - Feline Cardiology
P. 223
228 Section F: Arrhythmias and Other Electrocardiographic Abnormalities
V V V V T
QRS
P T
QRS
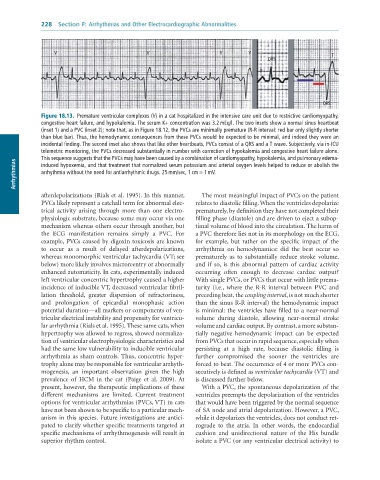
Figure 18.13. Premature ventricular complexes (V) in a cat hospitalized in the intensive care unit due to restrictive cardiomyopathy,
congestive heart failure, and hypokalemia. The serum K+ concentration was 3.2 mEq/l. The two insets show a normal sinus heartbeat
(inset 1) and a PVC (inset 2); note that, as in Figure 18.12, the PVCs are minimally premature (R-R interval: red bar only slightly shorter
than blue bar). Thus, the hemodynamic consequences from these PVCs would be expected to be minimal, and indeed they were an
incidental finding. The second inset also shows that like other heartbeats, PVCs consist of a QRS and a T wave. Subjectively, via in-ICU
telemetric monitoring, the PVCs decreased substantially in number with correction of hypokalemia and congestive heart failure alone.
This sequence suggests that the PVCs may have been caused by a combination of cardiomyopathy, hypokalemia, and pulmonary edema-
Arrhythmias arrhythmia without the need for antiarrhythmic drugs. 25 mm/sec, 1 cm = 1 mV.
induced hypoxemia, and that treatment that normalized serum potassium and arterial oxygen levels helped to reduce or abolish the
afterdepolarizations (Rials et al. 1995). In this manner, The most meaningful impact of PVCs on the patient
PVCs likely represent a catchall term for abnormal elec- relates to diastolic filling. When the ventricles depolarize
trical activity arising through more than one electro- prematurely, by definition they have not completed their
physiologic substrate, because some may occur via one filling phase (diastole) and are driven to eject a subop-
mechanism whereas others occur through another, but timal volume of blood into the circulation. The harm of
the ECG manifestation remains simply a PVC. For a PVC therefore lies not in its morphology on the ECG,
example, PVCs caused by digoxin toxicosis are known for example, but rather on the specific impact of the
to occur as a result of delayed afterdepolarizations, arrhythmia on hemodynamics: did the beat occur so
whereas monomorphic ventricular tachycardia (VT; see prematurely as to substantially reduce stroke volume,
below) more likely involves microreentry or abnormally and if so, is this abnormal pattern of cardiac activity
enhanced automaticity. In cats, experimentally induced occurring often enough to decrease cardiac output?
left ventricular concentric hypertrophy caused a higher With single PVCs, or PVCs that occur with little prema-
incidence of inducible VT, decreased ventricular fibril- turity (i.e., where the R-R interval between PVC and
lation threshold, greater dispersion of refractoriness, preceding beat, the coupling interval, is not much shorter
and prolongation of epicardial monophasic action than the sinus R-R interval) the hemodynamic impact
potential duration—all markers or components of ven- is minimal: the ventricles have filled to a near-normal
tricular electrical instability and propensity for ventricu- volume during diastole, allowing near-normal stroke
lar arrhythmia (Rials et al. 1995). These same cats, when volume and cardiac output. By contrast, a more substan-
hypertrophy was allowed to regress, showed normaliza- tially negative hemodynamic impact can be expected
tion of ventricular electrophysiologic characteristics and from PVCs that occur in rapid sequence, especially when
had the same low vulnerability to inducible ventricular persisting at a high rate, because diastolic filling is
arrhythmia as sham controls. Thus, concentric hyper- further compromised the sooner the ventricles are
trophy alone may be responsible for ventricular arrhyth- forced to beat. The occurrence of 4 or more PVCs con-
mogenesis, an important observation given the high secutively is defined as ventricular tachycardia (VT) and
prevalence of HCM in the cat (Paige et al. 2009). At is discussed further below.
present, however, the therapeutic implications of these With a PVC, the spontaneous depolarization of the
different mechanisms are limited. Current treatment ventricles preempts the depolarization of the ventricles
options for ventricular arrhythmias (PVCs, VT) in cats that would have been triggered by the normal sequence
have not been shown to be specific to a particular mech- of SA node and atrial depolarization. However, a PVC,
anism in this species. Future investigations are antici- while it depolarizes the ventricles, does not conduct ret-
pated to clarify whether specific treatments targeted at rograde to the atria. In other words, the endocardial
specific mechanisms of arrhythmogenesis will result in cushion and unidirectional nature of the His bundle
superior rhythm control. isolate a PVC (or any ventricular electrical activity) to