
Page 226 - Feline Cardiology
P. 226
Chapter 18: Arrhythmias and Other Electrocardiographic Abnormalities 231
according to site of origin: a PVC that begins in the left inaccurate prognosis, or otherwise bring harm. The dif-
ventricular free wall spreads toward the right, a very ferential diagnosis for wide, bizarre QRS complexes on
different pattern from normal, resulting in a very wide an ECG consists of
and different-appearing QRS complex. By contrast, a
PVC that originates near the point of entry of the His • Premature ventricular complex/ventricular tachycardia/
bundle into the ventricles (e.g., base of the right ven- AV dissociation with accelerated junctional rhythm
tricle) may spread through the ventricles in a manner • Ventricular escape rhythm (Figure 18.20)
not substantially different from normal depolarization, • Sinus rhythm with right or left bundle branch block
and the morphology of such a PVC is only mildly dif- or fascicular block (Figure 18.22)
ferent from the normal QRS complex (see Figure 18.12). • Right axis deviation due to right ventricular enlarge-
Several electrocardiographic impostors exist that ment or displacement of the heart (Figure 18.16)
mimic PVCs (Figures 18.14–18.16; see also Figures • Accelerated idioventricular rhythm (Figure 18.15)
18.20a, 18.22, 18.24–18.27, later in this chapter). • Motion artifact (Figure 18.14)
Therefore it is essential to accurately identify PVCs as • Hyperkalemia (Figures 18.24, 18.25)
such, because misdiagnosis may lead to treatment that • Macroreentrant tachycardia (preexcitation) (Figure
worsens rather than helps the patient, convey a grossly 18.27) Arrhythmias
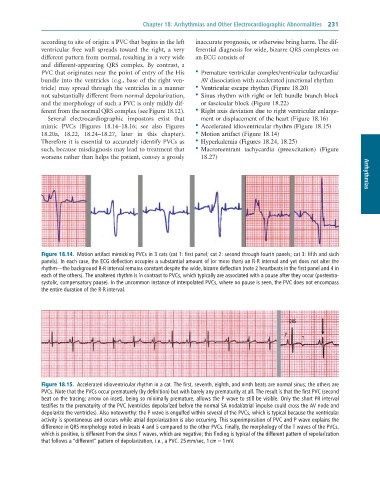
Figure 18.14. Motion artifact mimicking PVCs in 3 cats (cat 1: first panel; cat 2: second through fourth panels; cat 3: fifth and sixth
panels). In each case, the ECG deflection occupies a substantial amount of (or more than) an R-R interval and yet does not alter the
rhythm—the background R-R interval remains constant despite the wide, bizarre deflection (note 2 heartbeats in the first panel and 4 in
each of the others). The unaltered rhythm is in contrast to PVCs, which typically are associated with a pause after they occur (postextra-
systolic, compensatory pause). In the uncommon instance of interpolated PVCs, where no pause is seen, the PVC does not encompass
the entire duration of the R-R interval.
QRS
P
T
Figure 18.15. Accelerated idioventricular rhythm in a cat. The first, seventh, eighth, and ninth beats are normal sinus; the others are
PVCs. Note that the PVCs occur prematurely (by definition) but with barely any prematurity at all. The result is that the first PVC (second
beat on the tracing; arrow on inset), being so minimally premature, allows the P wave to still be visible. Only the short PR interval
testifies to the prematurity of the PVC (ventricles depolarized before the normal SA nodal/atrial impulse could cross the AV node and
depolarize the ventricles). Also noteworthy: the P wave is engulfed within several of the PVCs, which is typical because the ventricular
activity is spontaneous and occurs while atrial depolarization is also occurring. This superimposition of PVC and P wave explains the
difference in QRS morphology noted in beats 4 and 5 compared to the other PVCs. Finally, the morphology of the T waves of the PVCs,
which is positive, is different from the sinus T waves, which are negative; this finding is typical of the different pattern of repolarization
that follows a “different” pattern of depolarization, i.e., a PVC. 25 mm/sec, 1 cm = 1 mV.