
Page 233 - Manual of Equine Field Surgery
P. 233
Third-Degree Perinea! Laceration Repair 229
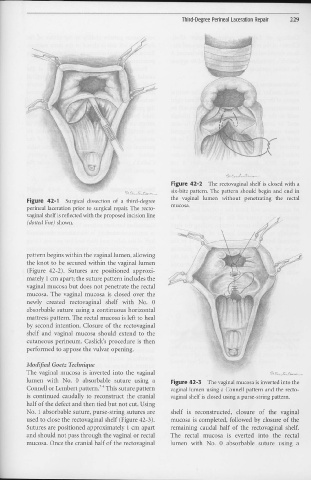
Figure 42-2 The rectovaginal shelf is closed with a
six-bite pattern. The pattern should begin and end in
Figure 42-1 Surgical dissection of a third-degree the vaginal lumen without penetrating the rectal
perinea! laceration prior to surgical repair. The recto- mucosa.
vaginal shelf is reflected with the proposed incision line
(dotted line) shown.
·-
-"-··- -c-, .... ~ ..
pattern begins within the vaginal lumen, allowing
the knot to be secured within the vaginal lumen
(Figure 42-2). Sutures are positioned approxi-
mately 1 cm apart; the suture pattern includes the
vaginal 1n11cosa but does not penetrate the rectal
mucosa. The vaginal mucosa is closed over the
newly created rectovaginal shelf with No. 0
absorbable suture using a continuous horizontal
mattress pattern. The rectal mucosa is left to heal
by second intention. Closure of the rectovaginal
shelf and vaginal mucosa should extend to the
cutaneous perineum. Caslick's procedure is then
performed to appose the vulvar opening.
Modified Goetz Technique
The vaginal mucosa is inverted into the vaginal
lumen with No. 0 absorbable suture using a Figure 42-3 The vaginal mucosa is inverted into the
Connell or Lembert pattem.i" This suture pattern vaginal lumen using a Connell pattern and the recto-
is continued caudally to reconstruct the cranial vaginal shelf is closed using a purse-string pattern,
half of the defect and then tied but not cut. Using
No. 1 absorbable suture, purse-string sutures are shelf is reconstructed, closure of the vaginal
used to close the rectovaginal shelf (Figure 42-3). mucosa is completed, followed by closure of the
Sutures are positioned approximately 1 cm apart remaining caudal half of the rectovaginal shelf.
and should not pass through the vaginal or rectal The rectal mucosa is everted into the rectal
mucosa. Once the cranial half of the rectovaginal lumen with No. 0 absorbable suture using a