
Page 701 - outbind://23/
P. 701
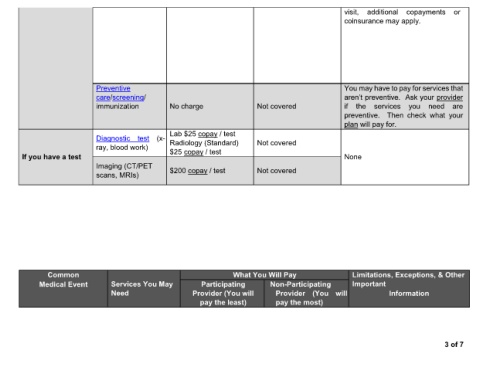
visit, additional copayments or
coinsurance may apply.
Preventive You may have to pay for services that
care/screening/ provider
immunization No charge Not covered if the services you need are
preventive. Then check what your
plan will pay for.
Lab $25 copay / test
Diagnostic test (x-
ray, blood work) Radiology (Standard) Not covered
If you have a test $25 copay / test None
Imaging (CT/PET $200 copay / test Not covered
scans, MRIs)
Common What You Will Pay Limitations, Exceptions, & Other
Medical Event Services You May Participating Non-Participating Important
Need Provider (You will Provider (You will Information
pay the least) pay the most)
3 of 7