
Page 702 - outbind://23/
P. 702
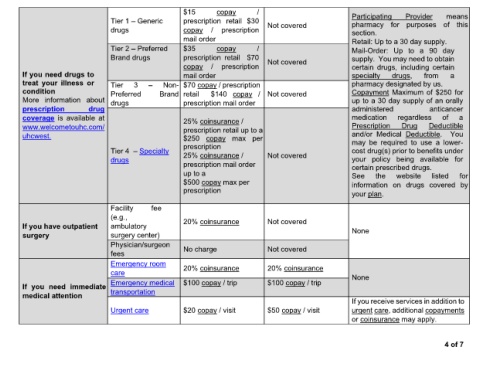
$15 copay / Participating Provider means
Tier 1 Generic prescription retail $30 Not covered pharmacy for purposes of this
drugs copay / prescription section.
mail order Retail: Up to a 30 day supply.
Tier 2 Preferred $35 copay / Mail-Order: Up to a 90 day
Brand drugs prescription retail $70 Not covered supply. You may need to obtain
copay / prescription certain drugs, including certain
If you need drugs to mail order specialty drugs, from a
treat your illness or Tier 3 Non- $70 copay / prescription pharmacy designated by us.
condition Preferred Brand retail $140 copay / Not covered Copayment Maximum of $250 for
More information about drugs prescription mail order up to a 30 day supply of an orally
prescription drug administered anticancer
coverage is available at 25% coinsurance / medication regardless of a
www.welcometouhc.com/ prescription retail up to a Prescription Drug Deductible
uhcwest. $250 copay max per and/or Medical Deductible. You
prescription may be required to use a lower-
Tier 4 Specialty 25% coinsurance / cost drug(s) prior to benefits under
drugs Not covered your policy being available for
prescription mail order certain prescribed drugs.
up to a See the website listed for
$500 copay max per information on drugs covered by
prescription your plan.
Facility fee
(e.g.,
If you have outpatient ambulatory 20% coinsurance Not covered None
surgery surgery center)
Physician/surgeon No charge Not covered
fees
Emergency room
care 20% coinsurance 20% coinsurance None
Emergency medical $100 copay / trip $100 copay / trip
If you need immediate
medical attention transportation
If you receive services in addition to
Urgent care $20 copay / visit $50 copay / visit urgent care, additional copayments
or coinsurance may apply.
4 of 7