
Page 4 - Benefit Guide_SIPS_2020_Revised 2-12-21
P. 4
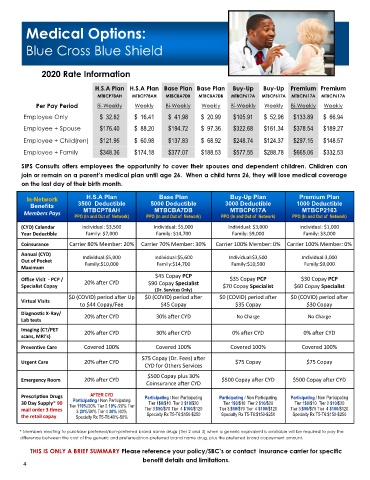
Medical Options:
Blue Cross Blue Shield
2020 Rate Information
H.S.A Plan H.S.A Plan Base Plan Base Plan Buy-Up Buy-Up Premium Premium
MTBCP78AH MTBCP78AH MTBCBA7DB MTBCBA7DB MTBCP617A MTBCP617A MTBCP617A MTBCP617A
Per Pay Period Bi-Weekly Weekly Bi-Weekly Weekly Bi-Weekly Weekly Bi-Weekly Weekly
Employee Only $ 32.82 $ 16.41 $ 41.98 $ 20.99 $105.91 $ 52.96 $133.89 $ 66.94
Employee + Spouse $176.40 $ 88.20 $194.72 $ 97.36 $322.68 $161.34 $378.54 $189.27
Employee + Child(ren) $121.95 $ 60.98 $137.83 $ 68.92 $248.74 $124.37 $297.15 $148.57
Employee + Family $348.36 $174.18 $377.07 $188.53 $577.55 $288.78 $665.06 $332.53
SIPS Consults offers employees the opportunity to cover their spouses and dependent children. Children can
join or remain on a parent’s medical plan until age 26. When a child turns 26, they will lose medical coverage
on the last day of their birth month.
In-Network H.S.A Plan Base Plan Buy-Up Plan Premium Plan
Benefits 3500 Deductible 5000 Deductible 3000 Deductible 1000 Deductible
Members Pays MTBCP78AH MTBCBA7DB MTBCP617A MTBCP2163
PPO (In and Out of Network) PPO (In and Out of Network) PPO (In and Out of Network) PPO (In and Out of Network)
(CYD) Calendar Individual: $3,500 Individual: $5,000 Individual: $3,000 Individual: $1,000
Year Deductible Family: $7,000 Family: $14,700 Family: $9,000 Family: $3,000
Coinsurance Carrier 80% Member: 20% Carrier 70% Member: 30% Carrier 100% Member: 0% Carrier 100% Member: 0%
Annual (CYD)
Individual:$5,000 Individual:$5,600 Individual:$3,500 Individual:3,000
Out of Pocket Family:$10,000 Family:$14,700 Family:$10,500 Family:$9,000
Maximum
$45 Copay PCP
Office Visit - PCP / 20% after CYD $35 Copay PCP $30 Copay PCP
Specialist Copay $90 Copay Specialist $70 Copay Specialist $60 Copay Specialist
(Dr. Services Only)
$0 (COVID) period after Up $0 (COVID) period after $0 (COVID) period after $0 (COVID) period after
Virtual Visits
to $44 Copay/Fee $45 Copay $35 Copay $30 Copay
Diagnostic X-Ray/ 20% after CYD 30% after CYD No Charge No Charge
Lab tests
Imaging (CT/PET 20% after CYD 30% after CYD 0% after CYD 0% after CYD
scans, MRI’s)
Preventive Care Covered 100% Covered 100% Covered 100% Covered 100%
$75 Copay (Dr. Fees) after
Urgent Care 20% after CYD $75 Copay $75 Copay
CYD for Others Services
$500 Copay plus 30%
Emergency Room 20% after CYD $500 Copay after CYD $500 Copay after CYD
Coinsurance after CYD
Prescription Drugs AFTER CYD Participating / Non Participating ticipating / Non Participating cipating / Non Participating
r
t
P
a
r
i
a
P
Participating / Non Participating
30 Day Supply* 90 Tier 110%/20% Tier 2 10% /20% Tier Tier 1$0/$10 Tier 2 $10/$20 Tier 1$0/$10 Tier 2 $10/$20 Tier 1$0/$10 Tier 2 $10/$20
mail order 3 times 3 20%/30% Tier 4 30% /40% Tier 3:$50/$70 Tier 4 $100/$120 Tier 3:$50/$70 Tier 4 $100/$120 Tier 3:$50/$70 Tier 4 $100/$120
the retail copay Specialty Rx T5-T6:40%-50% Specialty Rx T5-T6:$150-$250 Specialty Rx T5-T6:$150-$250 Specialty Rx T5-T6:$150-$250
* Members electing to purchase preferred/non-preferred brand name drugs (Tier 2 and 3) when a generic equivalent is available will be required to pay the
difference between the cost of the generic and preferred/non-preferred brand name drug, plus the preferred brand copayment amount.
THIS IS ONLY A BRIEF SUMMARY Please reference your policy/SBC’s or contact insurance carrier for specific
benefit details and limitations.
4