
Page 5 - 2020 McLennan County Benefits Enrollment Guide
P. 5
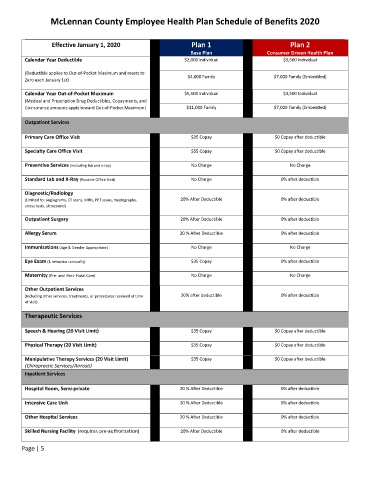
McLennan County Employee Health Plan Schedule of Benefits 2020
Effective January 1, 2020 Plan 1 Plan 2
Base Plan Consumer Driven Health Plan
Calendar Year Deductible $2,000 Individual $3,500 Individual
(Deductible applies to Out-of-Pocket Maximum and resets to
Zero each January 1st) $4,000 Family $7,000 Family (Embedded)
Calendar Year Out-of-Pocket Maximum $5,500 Individual $3,500 Individual
(Medical and Prescription Drug Deductibles, Copayments, and
Coinsurance amounts apply toward Out-of-Pocket Maximum) $11,000 Family $7,000 Family (Embedded)
Outpatient Services
Primary Care Office Visit $35 Copay $0 Copay after deductible
Specialty Care Office Visit $55 Copay $0 Copay after deductible
Preventive Services (including lab and x-ray) No Charge No Charge
Standard Lab and X-Ray (Routine Office Visit) No Charge 0% after deductible
Diagnostic/Radiology
(Limited to: angiograms, CT scans, MRIs, PET scans, myelography, 20% After Deductible 0% after deductible
stress tests, ultrasound)
Outpatient Surgery 20% After Deductible 0% after deductible
Allergy Serum 20 % After Deductible 0% after deductible
Immunizations (Age & Gender Appropriate) No Charge No Charge
Eye Exam (1 refraction annually) $35 Copay 0% after deductible
Maternity (Pre- and Post- Natal Care) No Charge No Charge
Other Outpatient Services
(Including other services, treatments, or procedures received at time 20% after deductible 0% after deductible
of visit)
Therapeutic Services
Speech & Hearing (20 Visit Limit) $35 Copay $0 Copay after deductible
Physical Therapy (20 Visit Limit) $35 Copay $0 Copay after deductible
Manipulative Therapy Services (20 Visit Limit) $35 Copay $0 Copay after deductible
(Chiropractic Services/Airrosti)
Inpatient Services
Hospital Room, Semi-private 20 % After Deductible 0% after deductible
Intensive Care Unit 20 % After Deductible 0% after deductible
Other Hospital Services 20 % After Deductible 0% after deductible
Skilled Nursing Facility (requires pre-authorization) 20% After Deductible 0% after deductible
Page | 5