
Page 7 - 2020 McLennan County Benefits Enrollment Guide
P. 7
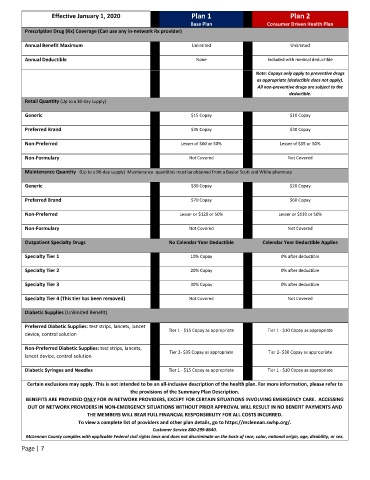
Effective January 1, 2020 Plan 1 Plan 2
Base Plan Consumer Driven Health Plan
Prescription Drug (Rx) Coverage (Can use any in-network Rx provider)
Annual Benefit Maximum Unlimited Unlimited
Annual Deductible None Included with medical deductible
Note: Copays only apply to preventive drugs
as appropriate (deductible does not apply).
All non-preventive drugs are subject to the
deductible.
Retail Quantity (Up to a 30-day supply)
Generic $10 Copay
$15 Copay
Preferred Brand $35 Copay $30 Copay
Non-Preferred Lesser of $60 or 50% Lesser of $55 or 50%
Non-Formulary Not Covered Not Covered
Maintenance Quantity (Up to a 90-day supply) Maintenance quantities must be obtained from a Baylor Scott and White pharmacy
Generic $20 Copay
$30 Copay
Preferred Brand $70 Copay $60 Copay
Non-Preferred Lesser or $120 or 50% Lesser or $110 or 50%
Non-Formulary Not Covered Not Covered
Outpatient Specialty Drugs No Calendar Year Deductible Calendar Year Deductible Applies
Specialty Tier 1 10% Copay 0% after deductible
Specialty Tier 2 20% Copay 0% after deductible
Specialty Tier 3 30% Copay 0% after deductible
Specialty Tier 4 (This tier has been removed) Not Covered Not Covered
Diabetic Supplies (Unlimited Benefit)
Preferred Diabetic Supplies: test strips, lancets, lancet
device, control solution Tier 1 - $15 Copay as appropriate Tier 1 - $10 Copay as appropriate
Non-Preferred Diabetic Supplies: test strips, lancets,
lancet device, control solution Tier 2- $35 Copay as appropriate Tier 2- $30 Copay as appropriate
Diabetic Syringes and Needles Tier 1 - $15 Copay as appropriate Tier 1 - $10 Copay as appropriate
Certain exclusions may apply. This is not intended to be an all-inclusive description of the health plan. For more information, please refer to
the provisions of the Summary Plan Description.
BENEFITS ARE PROVIDED ONLY FOR IN NETWORK PROVIDERS, EXCEPT FOR CERTAIN SITUATIONS INVOLVING EMERGENCY CARE. ACCESSING
OUT OF NETWORK PROVIDERS IN NON-EMERGENCY SITUATIONS WITHOUT PRIOR APPROVAL WILL RESULT IN NO BENEFIT PAYMENTS AND
THE MEMBERS WILL BEAR FULL FINANCIAL RESPONSIBILITY FOR ALL COSTS INCURRED.
To view a complete list of providers and other plan details, go to https://mclennan.swhp.org/.
Customer Service 800-299-8640.
McLennan County complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
Page | 7