
Page 12 - Deweys Benefits Enrollments Guide
P. 12
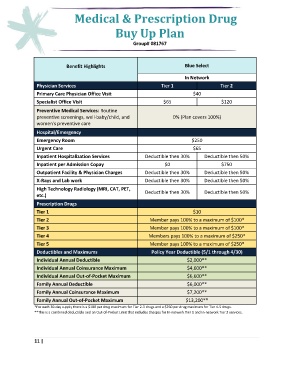
Medical & Prescription Drug
Buy Up Plan
Group# 081767
Benefit Highlights Blue Select
In Network
Physician Services Tier 1 Tier 2
Primary Care Physician Office Visit $40
Specialist Office Visit $65 $120
Preventive Medical Services: Routine
preventive screenings, well-baby/child, and 0% (Plan covers 100%)
women's preventive care
Hospital/Emergency
Emergency Room $250
Urgent Care $65
Inpatient Hospitalization Services Deductible then 30% Deductible then 50%
Inpatient per Admission Copay $0 $750
Outpatient Facility & Physician Charges Deductible then 30% Deductible then 50%
X-Rays and Lab work Deductible then 30% Deductible then 50%
High Technology Radiology (MRI, CAT, PET,
etc.) Deductible then 30% Deductible then 50%
Prescription Drugs
Tier 1 $10
Tier 2 Member pays 100% to a maximum of $100*
Tier 3 Member pays 100% to a maximum of $100*
Tier 4 Members pays 100% to a maximum of $250*
Tier 5 Member pays 100% to a maximum of $250*
Deductibles and Maximums Policy Year Deductible (5/1 through 4/30)
Individual Annual Deductible $2,000**
Individual Annual Coinsurance Maximum $4,600**
Individual Annual Out-of-Pocket Maximum $6,600**
Family Annual Deductible $6,000**
Family Annual Coinsurance Maximum $7,200**
Family Annual Out-of-Pocket Maximum $13,200**
*For each 30-day supply there is a $100 per drug maximum for Tier 2-3 drugs and a $250 per drug maximum for Tier 4-5 drugs.
**This is a combined deductible and an Out-of-Pocket Limit that includes charges for In-network Tier 1 and In-network Tier 2 services.
11 |