
Page 18 - Deweys Benefits Enrollments Guide
P. 18
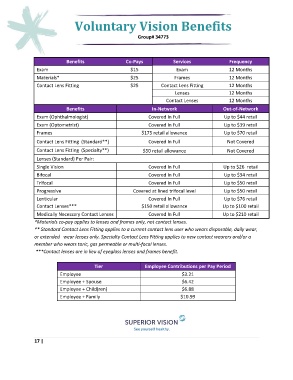
Voluntary Vision Benefits
Group# 34773
Benefits Co-Pays Services Frequency
Exam $15 Exam 12 Months
Materials* $25 Frames 12 Months
Contact Lens Fitting $25 Contact Lens Fitting 12 Months
Lenses 12 Months
Contact Lenses 12 Months
Benefits In-Network Out-of-Network
Exam (Ophthalmologist) Covered In Full Up to $44 retail
Exam (Optometrist) Covered In Full Up to $39 retail
Frames $175 retail allowance Up to $70 retail
Contact Lens Fitting (Standard**) Covered In Full Not Covered
Contact Lens Fitting (Specialty**) $50 retail allowance Not Covered
Lenses (Standard) Per Pair:
Single Vision Covered In Full Up to $26 retail
Bifocal Covered In Full Up to $34 retail
Trifocal Covered In Full Up to $50 retail
Progressive Covered at lined trifocal level Up to $50 retail
Lenticular Covered In Full Up to $76 retail
Contact Lenses*** $150 retail allowance Up to $100 retail
Medically Necessary Contact Lenses Covered In Full Up to $210 retail
*Materials co-pay applies to lenses and frames only, not contact lenses.
** Standard Contact Lens Fitting applies to a current contact lens user who wears disposable, daily wear,
or extended wear lenses only. Specialty Contact Lens Fitting applies to new contact wearers and/or a
member who wears toric, gas permeable or multi-focal lenses.
***Contact lenses are in lieu of eyeglass lenses and frames benefit.
Tier Employee Contributions per Pay Period
Employee $3.21
Employee + Spouse $6.42
Employee + Child(ren) $6.88
Employee + Family $10.99
17 |